PREOPERATIVE
PLANNING FOR RENAL CELL CARCINOMA - BENEFITS OF 64-SLICE CT IMAGING
(
Download pdf )
MANJIRI DIGHE, THOMAS TAKAYAMA, WILLIAM H. BUSH JR
Department of Radiology (MD, WHB), and Department of Surgery (TT), University of Washington Medical Center, Seattle, Washington, USA
ABSTRACT
Surgery
is the primary form of treatment in localized renal cell carcinoma. Adrenal-sparing
nephrectomy, laparoscopic nephrectomy and nephron-sparing partial nephrectomy
are growing trends for more limited surgical resection. Accurate preoperative
imaging is essential for planning the surgical approach. Multislice CT
and MR are regarded as the most efficient modalities for imaging renal
neoplasms. Development of faster CT systems like 64-slice CT with improved
resolution and capability to achieve isotropic reformats have significantly
enhanced the role of CT in imaging of renal neoplasms.
This review article describes the present
state, technique and benefits of 64-slice CT scanning in preoperative
planning for RCC.
Key
words: renal cell carcinoma; imaging, three-dimensional; surgery
Int Braz J Urol. 2007; 33: 305-12
INTRODUCTION
Renal
cell carcinoma (RCC) is the fifth most common cancer in adults and accounts
for 85% of all malignant tumors of the kidney (1). It represents 3% of
all male and 2% of female cancers. The incidence of RCC is 6.0 - 8.0 per
100,000 of the population (2). Surgery is the primary form of treatment
in localized renal cell carcinoma. In addition, adrenal-sparing nephrectomy,
laparoscopic nephrectomy and nephron-sparing partial nephrectomy are growing
trends for more limited surgical resection (3). The aims of preoperative
imaging are to characterize the lesion, identify accessory vessels, define
adjacent organ extension, identify lymph nodal or visceral metastases,
reliably predict the presence and extent of any thrombus in the renal
vein, vena cava and heart and evaluate the other kidney.
Multislice CT and MR are regarded as the
most effective modalities for imaging renal neoplasms. Development of
faster CT systems like the 64-slice CT scanner with improved resolution
and capability to achieve isotropic reformats have significantly enhanced
the role of CT in preoperative imaging of renal neoplasms.
IMAGING TECHNIQUE AND PROTOCOLS WITH 64 SLICE MULTIDETECTOR TECHNOLOGY
Helical
CT has dramatically refined the diagnostic evaluation of renal pathologic
conditions by allowing image acquisition through the entire kidney during
various phases of contrast enhancement after the administration of a single
bolus of intravenous contrast material (4-7). Multi-detector 64-slice
CT technology takes advantage of significantly reduced image acquisition
time for multi-phasic, thin-slice image acquisitions of the kidneys in
a single breath-hold with superior contrast bolus utilization.
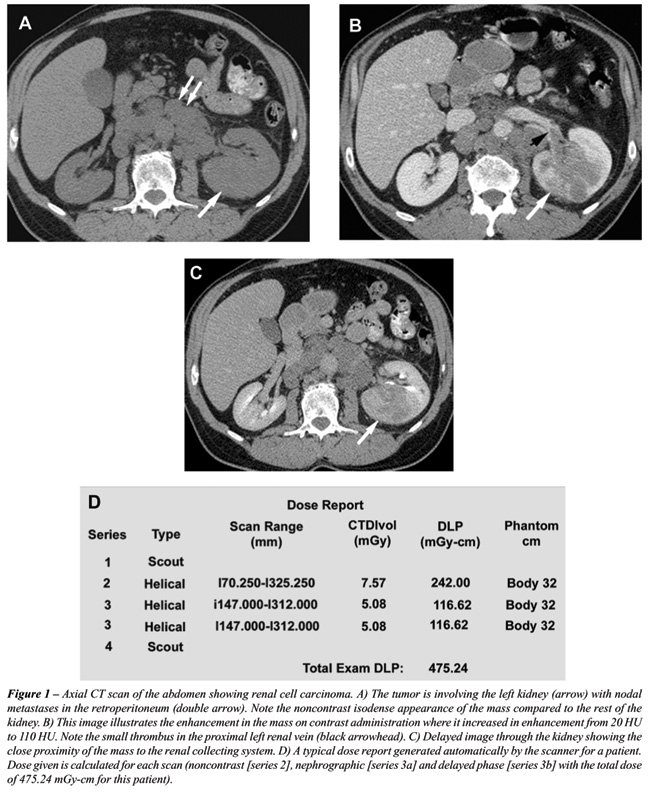
A precontrast phase provides a baseline
from which to measure the enhancement within the lesion after the administration
of intravenous contrast material. Calcifications are also seen in 30%
of cases of RCC. The enhancement characteristic is important in distinguishing
hyperdense cysts from solid tumors (Figures-1A and 1B). Because most renal
cell carcinomas have a rich vascular supply, they enhance significantly
after administration of intravascular contrast material. Enhancement values
of more than 15-20 HU are considered suspicious for malignancy (8); more
variation in enhancement is found with small masses due to the dense opacification
of adjacent normal parenchyma.
Generally, dual phase imaging with a nephrographic
phase and a delayed phase is used for evaluating suspected renal neoplasms
and depicting perinephric extension and vascular anatomy. For dual phase
imaging, 150 ml of non-ionic lower osmolality contrast media (320 mg ml-1)
is injected at 3 cc/sec and images are acquired following delays of approximately
90 seconds and 6 minutes for the nephrographic and pyelographic phases,
respectively. In some institutions, an initial scan is also performed
in the corticomedullary phase. In the corticomedullary phase, the contrast
material is primarily in the cortical capillaries, peritubular spaces,
and cortical tubular lamina and has not yet filtered through the more
distal renal tubules (9). In the nephrographic phase, the contrast material
filters through the glomeruli into the loops of Henle and collecting tubules
(9). The renal parenchyma enhances homogenously during this phase, due
to tubular accumulation. Renal tumors enhance less than the surrounding
parenchyma in this phase, because they lack normal glomerular-tubular
function and hence this phase is most valuable for detecting renal masses
and characterizing indeterminate lesions (10). The contrast reaches the
collecting system during the delayed or the excretory phase and, as a
result, the attenuation of the nephrogram progressively decreases (Figure-1C).
Macari & Bosniak (11) have suggested that measurement of the washout
of contrast material from a lesion at 15 minutes allows differentiation
between hyperdense cysts and renal neoplasms. In their study, there was
no change in the attenuation of high-density cysts between the initial
contrast-enhanced CT scan and the 15-minute-delayed images. In comparison,
all lesions that proved to be neoplasms at surgery or follow-up studies
showed a decrease in attenuation or “de-enhancement” of at
least 15 HU at delayed CT, which was attributed to the washout of contrast
material from the vascular bed of the tumor (11).
Contiguous thin sections are obtained using
protocols dependent on machine manufacturer to enable overlapping reconstruction.
At our institution, multiphase CT scans are obtained on GE Lightspeed
VCTTM 64 slice scanner at 0.625 mm thickness at a pitch of
1.375:1. These slices are reconstructed at 2.5 mm thickness in the axial
plane and coronal reformats are obtained at 5 mm intervals. Sagittal reformats
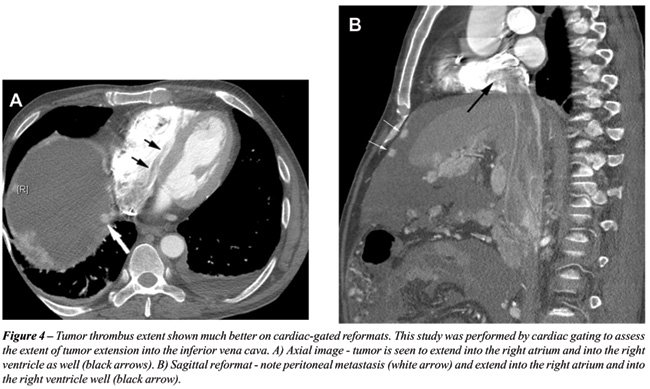
and 3D reconstruction are performed on a case specific basis. Cardiac
gated studies are performed for patients with IVC extension (see Figure-4).
Multi-phase CT of the abdomen is performed from top of the liver to 1
cm below the lowest kidney. A 15 minute scanogram is performed at the
end of the exam to assess the ureters. The protocol used at our institution
is illustrated in Table-1.
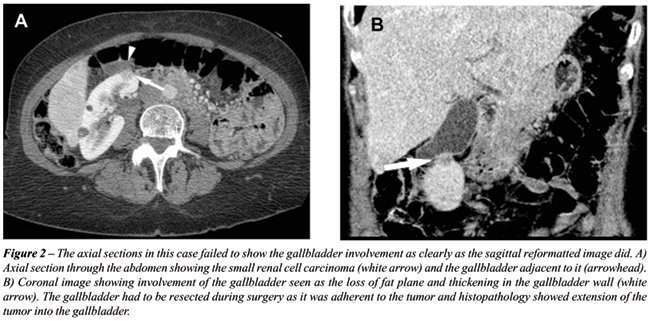
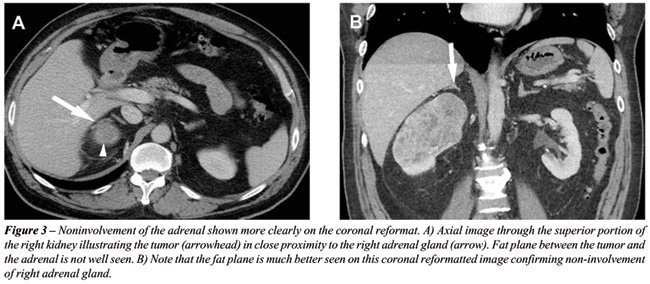
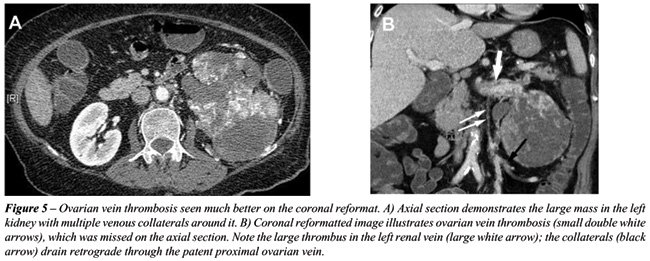
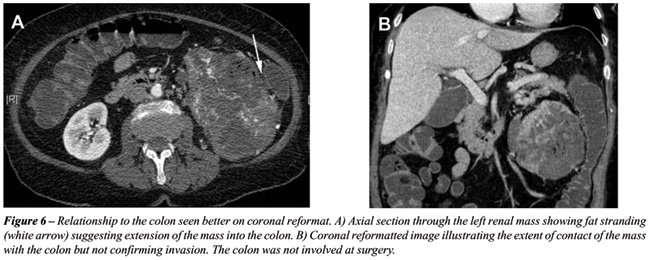
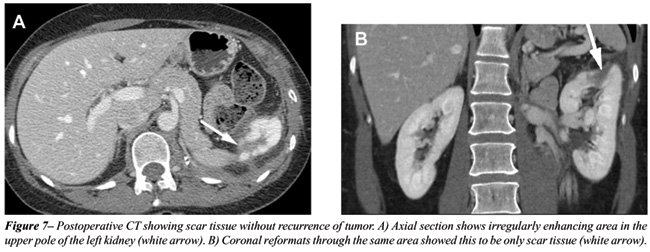
With the rapid acquisition of multiple simultaneous
slices and thin-section reformatted coronal and/or sagittal images, the
64-slice CT scanner provides excellent detail in demonstrating local extension
to the bowel and retroperitoneum (see Figures-2, 3, 5, 6 and 7). Multiplanar
three-dimensional reconstruction techniques including volume rendering,
maximum intensity projection and shaded surface display provide comprehensive
information about the relationships and possible involvement of vascular
structures in renal neoplasms.
TECHNICAL CONSIDERATIONS
Standard
oral contrast media for pre-operative assessment of renal neoplasm and
vasculature is unnecessary and may, in fact, obscure intravascular contrast.
The radiation dose in our CT scanners is regulated using the Smart mATM
feature, in which the mAs used is regulated according to the amount of
tissue (bone/soft tissue) that has to be traversed in x, y and z axes.
For example, the mAs used in the mid-abdomen is less than the mAs used
in the pelvis due to the bony structures in the pelvis. The radiation
dose given also depends on the patient’s size with more dose required
for larger patients and less for smaller patients. This is regulated according
to the body thickness as illustrated in Table-2. Maximum mAs to be used
can also be set in this Auto-mATM feature. Figure-1D illustrates
the average dose generated during each scan and the total dose report.
IMAGING AND SURGICAL PLANNING
Surgical
planning is usually enhanced by the information obtained from imaging
studies: extent of the tumor and its location in the kidney; proximity
to the renal collecting system and renal vessels; presence of fat planes
between the tumor and other structures (for e.g., liver, colon and posterior
abdominal wall muscles); tumor extension into the renal vein or IVC and
the level of this extension. The presence of intrabdominal metastasis,
the function of the contralateral kidney, and the appearance of the adrenal
glands are also reliably assessed (12), Tables-3 and 4.
CONCLUSION
64 slice CT imaging provides an improvement in the preoperative analysis of renal masses. The reformatted images in multiple planes and cardiac-gated sequences can offer additional help in surgical planning and reformatted images provide detailed information about arterial and venous collaterals and invasion of adjacent organs.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Heidenreich A, Ravery V, European Society of Oncological Urology: Preoperative imaging in renal cell cancer. World J Urol. 2004; 22: 307-5.
- Smith D: Renal Cancer. Urology. 2002; 20: 301-4.
- Russo P: Renal cell carcinoma: presentation, staging, and surgical treatment. Semin Oncol. 2000; 27: 160-76.
- Cohan RH, Sherman LS, Korobkin M, Bass JC, Francis IR: Renal masses: assessment of corticomedullary-phase and nephrographic-phase CT scans. Radiology. 1995; 196: 445-51.
- Kopka L, Fischer U, Zoeller G, Schmidt C, Ringert RH, Grabbe E: Dual-phase helical CT of the kidney: value of the corticomedullary and nephrographic phase for evaluation of renal lesions and preoperative staging of renal cell carcinoma. AJR Am J Roentgenol. 1997; 169: 1573-8.
- Szolar DH, Kammerhuber F, Altziebler S, Tillich M, Breinl E, Fotter R, et al.: Multiphasic helical CT of the kidney: increased conspicuity for detection and characterization of small (< 3-cm) renal masses. Radiology. 1997; 202: 211-7.
- Yuh BI, Cohan RH: Different phases of renal enhancement: role in detecting and characterizing renal masses during helical CT. AJR Am J Roentgenol. 1999; 173: 747-55.
- Israel GM, Bosniak MA: How I do it: evaluating renal masses. Radiology. 2005; 236: 441-50.
- Saunders HS, Dyer RB, Shifrin RY, Scharling ES, Bechtold RE, Zagoria RJ: The CT nephrogram: implications for evaluation of urinary tract disease. Radiographics. 1995; 15: 1069-85.
- Birnbaum BA, Jacobs JE, Ramchandani P: Multiphasic renal CT: comparison of renal mass enhancement during the corticomedullary and nephrographic phases. Radiology. 1996; 200: 753-8.
- Macari M, Bosniak MA: Delayed CT to evaluate renal masses incidentally discovered at contrast-enhanced CT: demonstration of vascularity with deenhancement. Radiology. 1999; 213: 674-80.
- Kaplan S, Ekici S, Dogan R, Demircin M, Ozen H, Pasaoglu I: Surgical management of renal cell carcinoma with inferior vena cava tumor thrombus. Am J Surg. 2002; 183: 292-9.
________
Accepted:
January 9, 2007
_______________________
Correspondence address:
Dr. Manjiri Dighe
Assistant Professor
Department of Radiology, Box 357115
University of Washington Medical Center,
Seattle, WA, 98195, USA
Fax: + 1 206 598-0252
E-mail: dighe@u.washington.edu