CONGENITAL
MEGAPREPUCE: A NEW ALTERNATIVE TECHNIQUE FOR SURGICAL CORRECTION
(
Download pdf )
JOVELINO Q. LEAO, LUIZ G. FREITAS FILHO, ADRIANO L. GOMES, ANTONIO C. HEINSICH, JOSE CARNEVALE
Division of Urology (JQL, LGFF, ALG, ACH, JC), Darcy Vargas Children’s Hospital, Sao Paulo, and Division of Pediatric Surgery (LGFF), Federal University of Sao Paulo, Sao Paulo, Brazil
ABSTRACT
Objective:
To present a new alternative technique for surgical treatment of congenital
megaprepuce.
Materials and Methods: From April 2004 to
April 2006, five patients aged 2 to 5 years were treated using the new
technique. The technique is described and illustrated. It differs from
other techniques in that it takes into consideration the constant ballooning
of the foreskin, which gives to the external genitalia the aspect of a
penoscrotal transposition. Cosmetic and functional success were also assessed
by a case review.
Results: After a follow-up of 1 to 3 years,
all patients have normal voiding and a satisfactory cosmetic aspect.
Conclusion: This new technique could be
a useful alternative in treatment of the congenital megaprepuce.
Key
words: penis; children; foreskin; congenital abnormalities; surgery
Int Braz J Urol. 2008; 34: 313-8
INTRODUCTION
Congenital
megaprepuce is a malformation consisting of a great redundancy of the
inner preputial skin over a normal penile shaft and glans. The prepuce
is not retractable and a ballooning of the foreskin is produced during
the micturition. It was first described by O’Brien et al., in 1994
(1), and, since then, other authors have shown that although a rare condition,
it is often confused with buried, trapped, concealed, webbed or micropenis
(1-3).
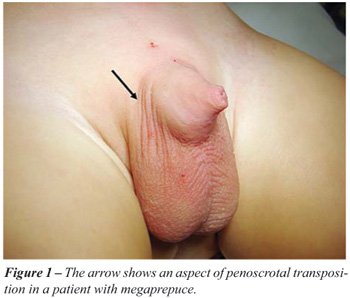
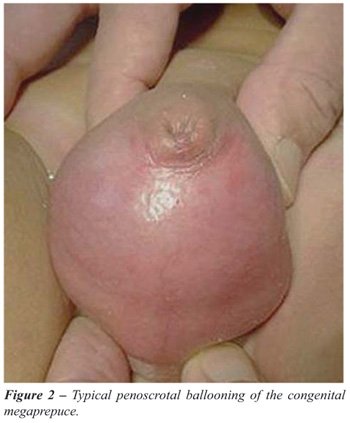
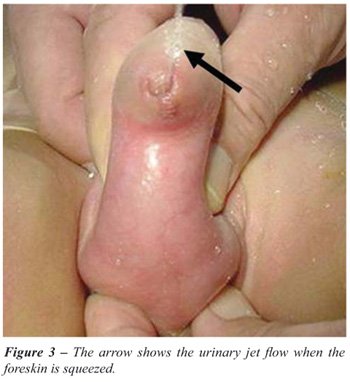
The exuberant inner prepuce closed by the
preputial ring creates a reservoir with a large dimension, leading to
the anatomical aspect of penoscrotal transposition (Figure-1 and 2). Compression
of the penile shaft results in urine spillage (Figure-3). The diagnosis
is made, therefore, essentially by physical examination, which does not
require functional exploration (4).
The objective of this report was to present
a new alternative surgical technique that takes in account the penoscrotal
transposition aspect of the malformation, which permits a satisfactory
cosmetic appearance.
MATERIALS AND METHODS
From
April 2004 to April 2006, five patients, aged 2 to 5 years, were treated
using the technique.
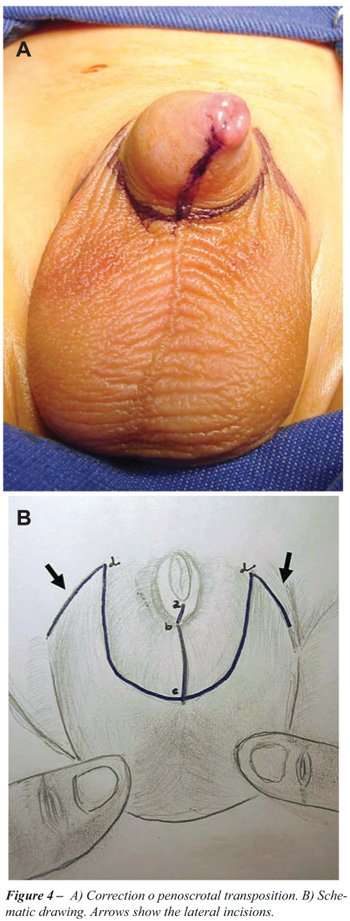
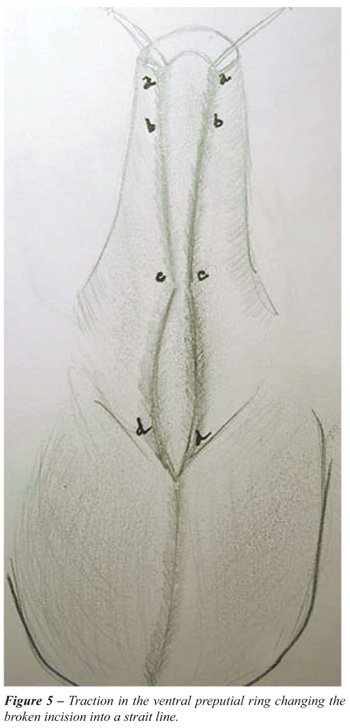
The initial skin incision is shown in Figure-4.
Then two traction stitches are made in the ventral point of the preputial
ring, disassembling the foreskin and penile shaft, transforming the broken
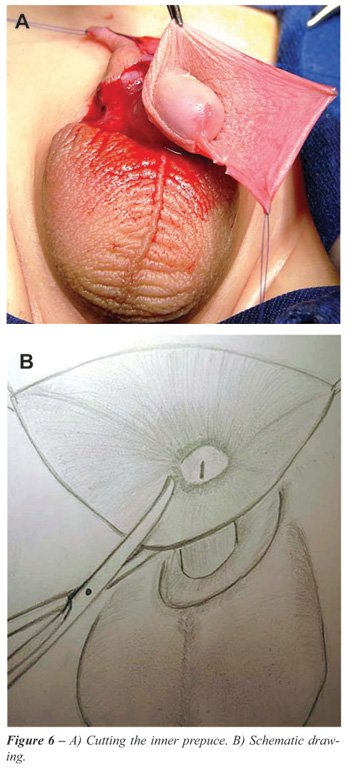
line incision in a vertical straight line, as shown in Figure-5. The inner
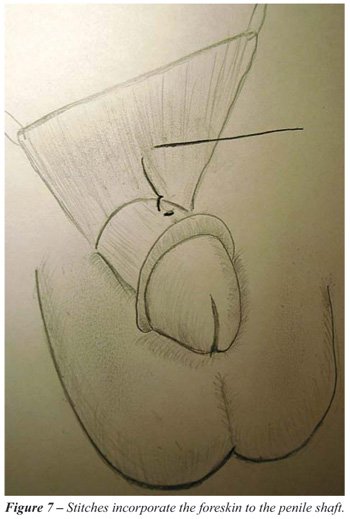
preputial skin is partially resected (Figure-6) and the foreskin is incorporated
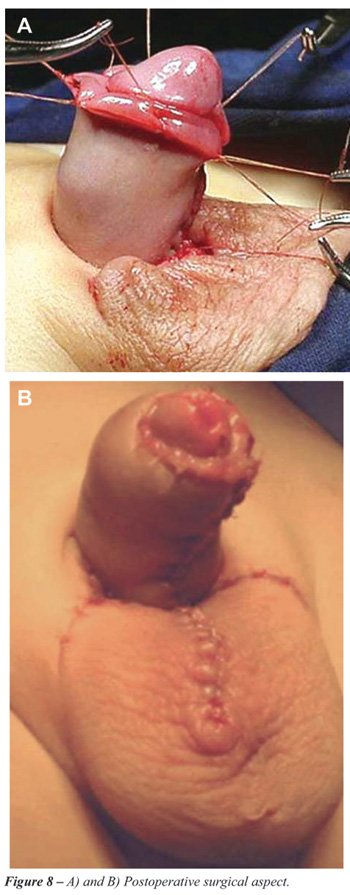
into the penile shaft with no flap required (Figure-7 and 8).
RESULTS
All
patients presented with the diagnosis of buried penis and 4 out of 5 have
had repeated urinary tract infections. After the surgical treatment all
patients have normal voiding pattern and the cosmetic aspect was considered
adequate 1 to 3 years after surgery (Figure-8 and 9).

COMMENTS
Congenital
megaprepuce was first described by O’Brien et al. (1). It is caused
by a redundant inner prepuce over a preputial ring, which is not retractable,
leading to a ballooning of the foreskin. Chronically it creates a reservoir,
which renders the external genitalia an aspect of a penoscrotal transposition.
In agreement with other authors we believe
that the condition is almost always confused with buried, trapped, concealed,
webbed or micropenis. We postulate, however, that other previously reported
surgical techniques have not considered the penoscrotal aspect of the
genitalia, chronically distended by the accumulation of urine (1-6) (Figures-2
and 3).
Unlike other published series all our patients
but one presented with a urinary tract infection (1-7).
As reported by Summerton et al. (3) we disagree
with Popis and Crapp (7) that early circumcision cures the problem because
this would remove the basic skin required to resurface the penile shaft.
The surgical technique presented in this
study is aimed at correcting the penoscrotal transposition in addition
to the resection of the redundant inner prepuce.
Although the present series included only
five patients, we believe, as in the series of Summerton et al. (3), that
when the immediate postoperative aspect is cosmetically treated, the long
term results will be satisfactory
CONFLICT OF INTEREST
None declared.
REFERENCES
- O’Brien A, Shapiro AMJ, Frank JD: Phimosis or congenital megaprepuce? Br J Urol 1994; 73:719-20.
- Shenoy MU, Rance CH: Surgical correction of congenital megaprepuce. Pediatr Surg Int. 1999; 15: 593-4.
- Summerton DJ, McNally J, Denny AJ, Malone PS: Congenital megaprepuce: an emerging condition--how to recognize and treat it. BJU Int. 2000; 86: 519-22.
- Delgado O, Dominguez H, Serrano D, Estornell M, Martinez V, Garcia I: Megaprepucio congenito: diagnostico y manejo terapeutico. Actas Urol Esp. 2006; 30: 1038-42.
- Philip I, Nicholas JL: Congenital giant prepucial sac: case reports.J Pediatr Surg. 1999; 34: 507-8.
- Ferro F, Spagnoli A, Spyridakis I, Atzori P, Martini L, Borsellino A: Surgical approach to the congenital megaprepuce. J Plast Reconstr Aesthet Surg. 2006; 59: 1453-7.
- Powis MR, Capps S: Preputial intussusception or acquired megaprepuce. Pediatr Surg Int. 1998; 13: 158-9.
____________________
Accepted after revision:
December 11, 2007
_______________________
Correspondence address:
Dr. Luiz G. Freitas Filho
Rua Batista Cepelos, 87 / 61
04109-120, São Paulo, SP, Brazil
E-mail: lfreitasf@terra.com.br