Anatrophic Nephrotomy as Nephron-Sparing Approach for Complete Removal of Intraparenchymal Renal Tumors
(Download pdf)
Marcos F. Dall'Oglio, Lucas Ballarotti, Carlo C. Passerotti, Davi V. Paluello, Jose Roberto Colombo Junior, Alexandre Crippa, Miguel Srougi
Urology Division, University of Sao Paulo Medical School, Sao Paulo, Brazil and Cancer Institute of Sao Paulo, Sao Paulo, Brazil
Original Article
Vol. 38 (3): 356-361; May - June, 2012
ABSTRACT
Purpose: Evaluate if the expression of metalloproteinase, collagen I and III could be related with Gleason score, preoperative PSA and pathological stage in prostate cancer.
Materials and Methods: Our study group included radical prostatectomy specimens of 33 patients with prostatic adenocarcinoma who underwent surgery from 2001 to 2009. Patients were divided into 3 groups: Gleason score=6 (13 patients), Gleason score=7 (10 patients), Gleason score≥8 (10 patients). The control group included prostates of patients submitted to cystoprostatectomy and benign prostatic tissues adjacent to the cancer area. Specific areas of tissues were selected under microscope and further processed for collagen I and III analysis by real time PCR. In addition, 10 deparaffined sections of each group were used to evaluate collagen I, III and metalloproteinase immunoexpression. The results were correlated with Gleason score, preoperative PSA and pathological stage.
Results: We found significant difference in both collagen I and III gene expression between benign and tumoral areas in the prostate samples from Gleason score=6 (collagen I=0.4±0.2 vs 5±2.4, p<0.05; collagen III=0.2±0.06 vs 0.7±0.1, p<0.05) and Gleason score≥8 (collagen I=8±3.4 vs 1.4±0.8, p<0.07; collagen III=1.8±0.5 vs 0.6±0.1, p<0.05). Nevertheless, there was no correlation of collagen expression with Gleason score, preoperative PSA or pathological stage. There was a positive correlation between metalloproteinase expression and Gleason score (r2=0.47).
Conclusions: The positive correlation between metalloproteinase expression and Gleason score suggests that metalloproteinase could be a promising factor to improve Gleason score evaluation. Its expression and regulation do not seem to be related with collagen degradation.
Key words: Kidney neoplasms; nephrons; Urologic Surgical Procedures; Outcome Assessment (Health Care)
INTRODUCTION
With the development of imaging diagnosis techniques, and the higher number of requested exams, there has been a growth of the incidence of small renal tumors, and an increase of the indication of nephron-sparing surgery, with excellent oncological and functional outcomes (1). In the last years, the incidental lesions are responsible for more than 60% of kidney tumors and 80% of these are in stages I and II (2).
Nephron-sparing renal surgery has been increasingly used for small renal mass (<4 cm) and, in selected cases, up to 7 cm renal tumors with similar oncological outcomes compared to radical nephrectomy, (3-5) with small complication ratio (6). The 5-year recurrence-free survival is approximately 96% for lesions smaller than 4 cm, and of 83% for lesions from 4 to 7 cm (7).
However, renal occult tumors diagnosed by imaging techniques represent greater technical difficulties for localization and resection, and may increase the chances of complications (8) (Figures 1A-C). To precisely locate the tumor during surgical resection, intraoperative ultrasound during the operation has been used successfully (9).
The objective of this study is to present an alternative surgical approach for the complete enucleation of endophytic tumors through anatrophic nephrotomy, avoiding radical nephrectomy.

MATERIALS AND METHODS
The authors performed a retrospective analysis of patients undergoing partial nephrectomy at their institution and all subjects with endophytic tumors treated with anatrophic nephrotomy were identified (Figures 2A-D). Patient demographics, perioperative, functional and oncologic results were evaluated. Among 554 renal tumors treated between 06/2006 and 06/2010, in 187 it was performed partial nephrectomy, and ten patients underwent partial nephrectomy through anatrophic nephrotomy.
The detailed operative technique is described below:
A) The access is made through either a flank or anterior subcostal incision; the kidney is dissected and exposed, and the renal artery and vein are repaired;
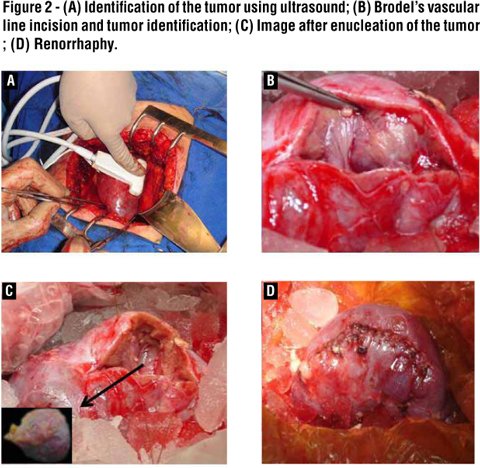
B) Ultrasound is used to identify the tumor borders and depth. Before renal artery clamping, it is infused intravenously 50 ml of mannitol 20% for nephron protection during warm ischemia. Ice is used to involve the kidney after clamping for 3 min before initiating the tumor resection, and in this case both artery and vein are clamped (Figure 2A);
C) Right after the renal artery clamping with a bulldog, the nephrotomy is performed along the Brodel’s vascular line for the visualization of the tumor (Figure 2B). The tumor enucleation is then carried out using a combination of blunt and sharp dissection (Figure 2C). The surgical specimen is immediately sent to the histopathological laboratory in order to verify the margins during the renal reconstruction. The hemostasis is done through parenchymal stitches of 2.0-chromed catgut. Renorrhaphy is then performed with a running Vicryl® 0 suture (Figure 2D);
D) A suction drain is placed surrounding the closed Gerota’s fascia in all cases and the incision is closed.
Results
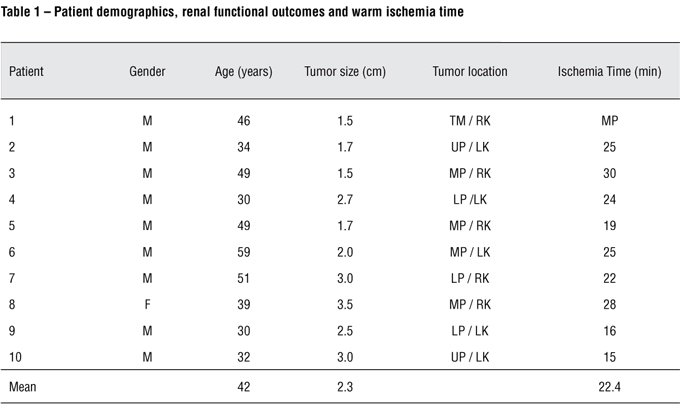
Ten patients were evaluated. The mean age was 42 yrs (30-59), and nine were male. The mean tumor size was 2.3 cm (1.5–3.5), compared with 3.5 + 2.4 cm of all partial nephrectomies. Mean warm ischemia time was 22.4 min (15-30) (Table 1). The mean pre-operative serum creatinine was 0.88 mg/dl, and the post-operative value was 0.94 mg/dl, measured two weeks after surgery.
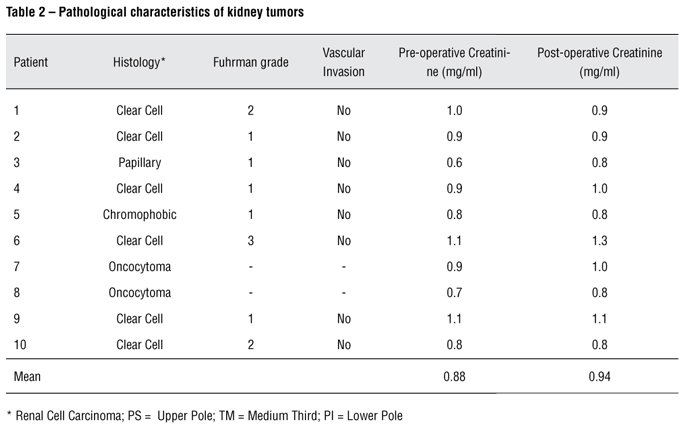
On the pathological analysis, two lesions had benign etiology (oncocytoma), and among the renal cell carcinomas, six were of clear cells, one papillary, and one chromophobic. The majority of the lesions were of low Fuhrman grade, and no positive surgical margin has been observed in this series (Table 2).
No patient showed significant intraoperative bleeding, with no blood transfusion, as well as urinary fistulas or collections. There was no loss of the renal unit in any patient submitted to surgery. All patients were monitored using the same protocol during a mean follow-up of 36 months (6–72), with no local recurrence or systemic metastatic disease observed.
Discussion
Anatrophic nephrotomy for handling solid and tumors completely endophytic represents a feasible approach for preservation of the kidney function in all cases, with adequate exposure and safety for tumor resection, as well as collector system closure and hemostasis.
Renal intraparenchymal (endophytic) tumors represent greater technical difficulties for localization and resection and may increase the chances of complications (8). Partial nephrectomy and/or enucleation represent 30% of the surgical procedures used for renal tumors, with long-term survival similar to radical nephrectomy for the initial stages, with cancer-specific and overall survival of 98% and 97% respectively (1,4,10). For tumors <4cm, there is no need to remove any additional surgical margin for optimal cancer control. The use of intraoperative ultrasound facilitates the precise identification of the lesion(s), its relation with intra-renal structures and the proximity of the major kidney vessels (9).
There are several definitions of central tumors, of which the best accepted are those of Black et al. (11), which consider that the lesion is completely surrounded by normal renal tissue, and that of Brown et al. (12) that define those with a distance shorter than 5 mm from the collection system or hilar vessels.
The anatrophic nephrectomy was developed for the treatment of staghorn lithiasis, with the opening of the renal parenchyma in the posterior face of the kidney under cold ischemia. Surgery studies targeting surgery for calculi occupying the entire collecting system show an average cold ischemia time varying from 20 to 45 minutes without significant blood loss (13, 14). Regarding the loss of renal function, the literature shows that 55% of the kidney units have their function maintained and just 13% exhibit a discrete reduction (13). The study of the relative function with DMSA shows an average reduction of 4% (15). Nohara et al. (15) described their technique for anatrophic partial nephrectomy with selective arterial clamping of the area of the tumor, after an angiography study, with a minor increase of the serum creatinine in the postoperative follow-up.
Nephron-sparing surgery for central but exophytic tumors has shown safety and efficacy compared to peripheral tumors. In a study with 118 patients, the operative and ischemia time, need of the closure of the collection system, and blood transfusion did not exhibit statistically differences (8). However, estimated blood loss was higher in the central tumor group: 220 ml (20 – 3500 ml) against 50 (5 to 1500 ml) in peripheral tumors. This same study showed a trend towards a higher number of urinomas and urinary fistulas in the central tumor group (8).
The technique presented herein allows a reliable approach, with a clear view of the tumors and their anatomical relations, with low complication rates (8, 6). Moreover, it is technically reproductible by the majority of urologists, because of their familiarity with the anatrophic nephrectomy technique used to remove large staghorn calculi. The mean ischemia time of 22.4 minutes is comparable to the time of the partial nephrectomy studies (8) and below the average of those of nephrotomies for treating calculi (13,14).
There is currently a growing use of minimally invasive ablative therapies for small kidney tumors, such as radiofrequency and cryotherapy, providing greater safety and expanding its indications. However, recent studies show a higher failure rate varying from 13% to 35% for RFA and 4% to 6% for cryoablation (16,17). The main factor for failures on procedures aided by laparoscopy is the endophytic nature of the lesions (8). Besides, there are no series for these types of treatments with patients that are so young such as those presented in this study, and with an adequate follow-up.
The limitations of the present study are represented by the small number of patients, with a median follow-up of 36 months and with no studies of the renal functions of the operated units other than serum creatinine. However, the lesions were safely enucleated and rendered negative margins, with acceptable warm ischemia time.
The nephron-sparing surgery for tumors completely endophytic through anatrophic nephrotomy was safe, with low complication rate and short warm ischemia time. It may be a reliable option when dealing with complex small kidney tumors.
Nowadays, the Urologists have the obligation to try to perform the nephron-sparing surgery in tumors <7cm, whenever possible (3-5). In particular, this study wants to reinforce the need for this strategy, since the partial open surgery is mandatory in these cases to avoid loss of renal unit in small (< 4 cm) and asymptomatic tumors.
CONFLICT OF INTEREST
None declared.
References
1. Riggs SB, Klatte T, Belldegrun AS. Update on partial nephrectomy and novel techniques. Urol Oncol. 2007; 25: 520-2.
2. Dall'Oglio M, Srougi M, Ortiz V, Nesrallah L, Gonçalves PD, Leite KM et al. [Incidental and symptomatic kidney cancer: pathological features and survival]. Rev Assoc Med Bras. 2004; 50: 27-31.
3. Mitchell RE, Gilbert SM, Murphy AM, Olsson CA, Benson MC, McKiernan JM. Partial nephrectomy and radical nephrectomy offer similar cancer outcomes in renal cortical tumors 4 cm or larger. Urology. 2006; 67: 260-4.
4. Ukimura O, Haber GP, Remer EM, Gill IS. Laparoscopic partial nephrectomy for incidental stage pT2 or worse tumors. Urology. 2006; 68: 976-82.
5. Leibovich BC, Blute ML, Cheville JC, Lohse CM, Weaver AL, Zincke H. Nephron sparing surgery for appropriately selected renal cell carcinoma between 4 and 7 cm results in outcome similar to radical nephrectomy. J Urol. 2004; 171: 1066-70.
6. Permpongkosol S, Link RE, Su LM, Romero FR, Bagga HS, Pavlovich CP et al. Complications of 2,775 urological laparoscopic procedures: 1993 to 2005. J Urol. 2007; 177: 580-5.
7. Patard JJ, Shvarts O, Lam JS, Pantuck AJ, Kim HL, Ficarra V et al. Safety and efficacy of partial nephrectomy for all T1 tumors based on an international multicenter experience. J Urol. 2004; 171: 2181-5.
8. Mullerad M, Kastin A, Adusumilli PS, Moskovitz B, Sabo E, Nativ O. Comparison of nephron-sparing surgery in central versus peripheral renal tumors. Urology. 2005; 65: 467-72.
9. Choyke PL, Pavlovich CP, Daryanani KD, Hewitt SM, Linehan WM, Walther MM. Intraoperative ultrasound during renal parenchymal sparing surgery for hereditary renal cancers: a 10-year experience. J Urol. 2001; 165: 397-400.
10. Herr HW. Partial nephrectomy for unilateral renal carcinoma and a normal contralateral kidney: 10-year followup. J Urol. 1999; 161: 33-4; discussion 34-5.
11. Black P, Filipas D, Fichtner J, Hohenfellner R, Thüroff JW. Nephron sparing surgery for central renal tumors: experience with 33 cases. J Urol. 2000; 163: 737-43.
12. Brown JA, Hubosky SG, Gomella LG, Strup SE. Hand assisted laparoscopic partial nephrectomy for peripheral and central lesions: a review of 30 consecutive cases. J Urol. 2004; 171: 1443-6.
13. Ramakrishnan PA, Al-Bulushi YH, Medhat M, Nair P, Mawali SG, Sampige VP. Modified anatrophic nephrolithotomy: A useful treatment option for complete complex staghorn calculi. Can J Urol. 2006; 13: 3261-70.
14. Morey AF, Nitahara KS, McAninch JW. Modified anatrophic nephrolithotomy for management of staghorn calculi: is renal function preserved? J Urol. 1999; 162: 670-3.
15. Nohara T, Fujita H, Yamamoto K, Kitagawa Y, Gabata T, Namiki M. Modified anatrophic partial nephrectomy with selective renal segmental artery clamping to preserve renal function: a preliminary report. Int J Urol. 2008; 15: 961-6.
16. Weight CJ, Kaouk JH, Hegarty NJ, Remer EM, O'Malley CM, Lane BR et al. Correlation of radiographic imaging and histopathology following cryoablation and radio frequency ablation for renal tumors. J Urol. 2008; 179: 1277-81; discussion 1281-3.
17. Matin SF, Ahrar K, Cadeddu JA, Gervais DA, McGovern FJ, Zagoria RJ et al. Residual and recurrent disease following renal energy ablative therapy: a multi-institutional study. J Urol. 2006; 176: 1973-7.
18. Wright AD, Turk TM, Nagar MS, Phelan MW, Perry KT. Endophytic lesions: a predictor of failure in laparoscopic renal cryoablation. J Endourol. 2007; 21: 1493-6.
________________
Submitted for publication:
March 23, 2011
________________
Accepted after revision:
April 18, 2012
_______________________
Correspondence address:
Dr. Marcos F. Dall'Oglio
Rua Barata Ribeiro, 398, 5º. Andar.
Sao Paulo, SP, 01308–000, Brazil.
Fax: + 55 11 3159-3618
E-mail: marcosdallogliouro@terra.com.br