THE
ACCURACY OF 99mTc-DTPA SCINTIGRAPHY IN THE EVALUATION OF ACUTE
RENAL GRAFT COMPLICATIONS
(
Download pdf )
ADELINA SANCHES, ELBA C.S.C. ETCHEBEHERE, MARILDA MAZZALI, G. ALVES FILHO, MARIANA C.L. LIMA, ALLAN O. SANTOS, CELSO D. RAMOS, IZILDA CARDINALLI, ATHANASE BILLIS, EDWALDO E. CAMARGO
Division of Nuclear Medicine, Department of Radiology, and Division of Nephrology, Department of Internal Medicine, and Department of Pathology, Campinas State University, UNICAMP, Campinas, São Paulo, Brazil
ABSTRACT
Purpose:
Renal scintigraphy has been used for many years in the evaluation of renal
transplants and can help in the diagnosis of graft complications, leading
to prompt clinical management and preventing further deterioration of
renal function. The purpose of this study was to evaluate the overall
accuracy of renal scintigraphy with 99mTc-DTPA in the diagnosis
of acute renal graft complications.
Materials and Methods: Seventy-six scintigraphic
studies performed in 55 patients (ages ranging from 6 to 65 years), were
reviewed. Scintigraphy results were compared to biopsies performed within
5 days of imaging. 99mTc-DTPA study was performed within a
mean time of 19 days after kidney transplants. Dynamic images were performed
in the anterior position of the abdomen and pelvis every 2 seconds for
80 seconds (flow phase) and every 15 seconds for 30 minutes (functional
phase), after an intravenous injection of 370 MBq (10 mCi) of 99mTc-DTPA.
Results: The scintigraphic results were
concordant with the biopsies in 86% of the cases studied. The sensitivities
of renal scintigraphy for detection of acute tubular necrosis (ATN), acute
rejection (AR) and cortical necrosis (CN) were 98%, 87% and 100%, respectively.
Specificities and accuracies for detection of ATN, AR and CN were 89%,
86% and 100%, and 95%, 87% and 100%, respectively.
Conclusion: Renal scintigraphy with 99mTc-DTPA
showed a good overall accuracy in the detection of acute renal graft complications.
It can be used as a reliable tool in the routine evaluation of these patients.
Key
words: kidney; kidney transplantation; radionuclide imaging;
graft rejection; diagnosis
Int Braz J Urol. 2003; 29: 507-516
INTRODUCTION
Renal
scintigraphy is one of the most frequently used methods in the evaluation
of renal allograft dysfunction (1-4) along with other diagnostic tests,
such as clinical criteria, ultrasound, serum creatinine levels, fine needle
aspiration biopsy, magnetic resonance imaging and core biopsy, helping
in the identification of acute and long term complications (5-7). The
most common renal transplant complications are acute tubular necrosis,
rejection (hyperacute, accelerated, acute, chronic), cyclosporin toxicity,
urine leak, hematoma, obstruction, lymphocele and renal artery stenosis.
Nuclear medicine plays an important role
in the investigation of renal graft complications and several radiopharmaceuticals
can be employed (8). Routinely, 99mTc-DTPA and 99mTc-MAG3
are used, although studies with 131I-OIH, 99mTc-GHA,
Ga-67, 99mTc-sulfur colloid, radiolabeled leukocytes and platelets
have also been performed (9-11). The scintigraphic evaluation of the transplanted
kidney involves qualitative or quantitative analysis of the 3 phases of
renal scintigraphy: the flow phase, the functional phase and the excretion
phase (4,12). 99mTc-DTPA can be very helpful in the evaluation
of dysfunctional kidneys, since it has a reasonable extraction rate and
a low cost.
Biopsy, the gold standard for the detection
of renal graft non-surgical complications, is an invasive procedure that
carries a higher morbidity when compared to non-invasive diagnostic tests
such as renal scintigraphy. Ideally, its use should be restricted to patients
in whom non-invasive procedures are indeterminate.
The purpose of this study was to determine
the accuracy of dynamic renal scintigraphy with 99mTc-DTPA
in the identification of acute renal graft complications, when compared
to core biopsy.
MATERIALS AND METHODS
Patient
Selection
Seventy-six
scintigraphic studies performed in 55 patients were reviewed. 99mTc-DTPA
study was performed 1 day to a maximum of 6 months (mean 19 days) after
kidney transplants (cadaveric or living donors).
Patients’ ages ranged from 6 to 65
years (mean 37 years), 38 were males (69%) and 49 (89%) were recipients
from cadaveric donors.
As part of the approach to transplanted
patients in our medical institution, they would undergo renal scintigraphy
routinely within the first 24 hours after surgery as a baseline study.
Studies were repeated whenever complications were suspected, so as biopsies
did, whenever clinically indicated. All patients in this study were retrospectively
collected when performed 99mTc-DTPA scintigraphy and core biopsies
within a maximum time interval of 5 days between the two procedures.
Other diagnostic methods such as urinary
outflow, creatinine levels, and Doppler ultrasound were performed whenever
necessary but not taken into analysis since it is not the aim of the present
study.
Renal
Scintigraphic Studies
Patients
received an intravenous injection of 370 MBq (10 mCi) of 99mTc–DTPA
and sequential images in the anterior position of the abdomen and pelvis,
every 2 seconds for 80 seconds (flow phase) and every 15 seconds for 30
minutes (functional phase) were begun immediately after injection.
Additional hydration prior to the study
was not addressed in the early days after transplantation since we did
not want to interfere in the water balance of the patients. Later, as
long as no restrictions advised by the referring physician, oral hydration
with 500 to 600 ml of water was given 30 minutes before the study.
Images were obtained on a camera-computer
system equipped with a LEAP collimator.
The flow and functional phases were analyzed
visually. Time-activity curves were also obtained from regions of interest
(ROI) drawn over the grafted kidney and the aorta, subtracting the background
activity.
Imaging
Interpretation
Three
experienced nuclear medicine physicians blindly interpreted the scintigraphies.
Scintigraphic criteria were pre-established and then compared to the biopsy
findings.
The blood flow phase was analyzed predominantly
qualitatively using the aorta or the iliac arteries as references. Renal
graft blood flow was considered normal when the peak kidney activity,
within 6 seconds of the peak aorta or iliac activity, was equal to or
higher than that of the peak aorta or iliac artery activity. Mildly, moderately
and severely decreased flow was considered as so according to the severity
of the flow reduction on the visual analysis as well.
Interpretation of the functional phase was
also performed qualitatively, evaluating the images and quantitatively,
evaluating the renogram curves. This evaluation included the accumulation
phase, in which the extraction of the tracer from the blood during the
first 3 minutes was evaluated; the concentration phase, in which the capacity
of concentrating urine (water absorption) was analyzed; and the excretion
phase, in which the transit of the radiopharmaceutical from the collecting
system to the bladder was evaluated.
According to the scintigraphic findings
in the flow and functional phases, the studies were classified as probable
acute tubular necrosis (ATN), acute rejection (AR), cortical necrosis
(CN), cyclosporin toxicity (CyT) and the association of ATN with AR (ATN
+ AR).
Scintigraphic
Criteria
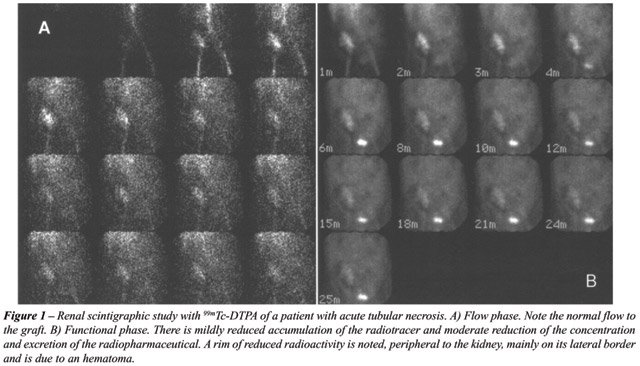
ATN
- Normal or mildly decreased blood flow; normal or mildly decreased accumulation
of the tracer, with a more prominent impairment of the concentration and
excretion phases (difficulty in progression of the tracer in the damaged
tubules) (Figure-1).
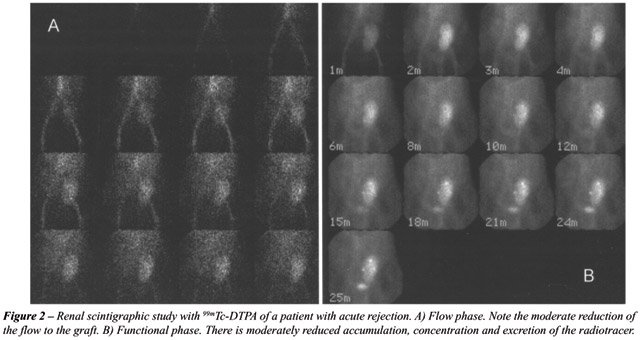
AR - Moderately or severely decreased blood
flow and function or significantly decreased renal blood flow and function
when compared to a previous study if available (Figure-2).
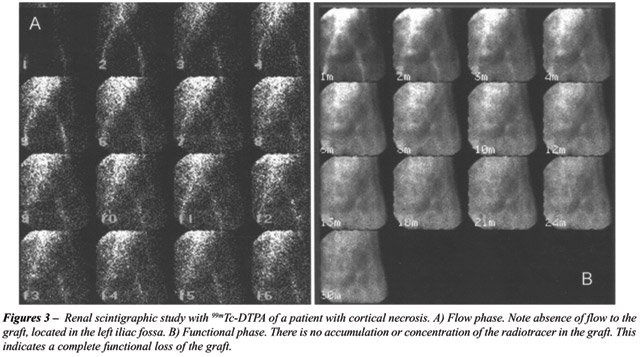
CN - Absence of blood flow and function,
the location of the graft depicted as a photopenic area (Figure-3).
CyT - Scintigraphic pattern similar to ATN.
Usually occurs after 30 days after the introduction of the drug, a period
during which the impairment in renal function caused by ATN is expected
to have subsided.
ATN + AR - Decreased flow and function in
the follow up studies of patients with previously detected ATN.
Histopathological
Analysis
Core
biopsy specimens were reviewed by an experienced pathologist according
to the Banff 97 criteria (13), using a 0 – 3 + semi quantitative
scale for each of the following histopathologic findings: acute glomerulitis,
lymphocytic tubulitis, interstitial inflammation, vasculitis, chronic
transplant glomerulopathy, interstitial fibrosis, tubular atrophy, and
fibrointimal thickening. Evidence for possible drug toxicity was also
recorded. Based on these findings, the biopsies were classified as ATN,
AR, ATN + AR, CN, CyT.
Statistical
Analysis
The
diagnostic value of scintigraphy was expressed as sensitivity (St), specificity
(Sp), positive predictive value (PPV), negative predictive value (NPV)
and accuracy (A) for the diagnosis of ATN, AR and CN. Biopsy was considered
the gold standard for comparison.
RESULTS
The
scintigraphic and biopsy results were compared and classified as concordant
or discordant (Table-1).
Scintigraphy identified 27 ATN, 45 AR and
4 CN events. Core biopsy identified 24 ATN, 47 AR, 4 CN and 1 CyT events.
Table-2 shows that 66 diagnoses (87%) were concordant and 10 (13%) were
discordant (Figure-4).
Among the 10 discordant studies, in 6 scintigraphy
failed to demonstrate AR detected by biopsy. In 4 cases, DTPA-99mTc
scintigraphy was interpreted as AR but biopsy showed only ATN in 3 cases
and CyT in the remainder.
Sensitivity, specificity, positive predictive
value, negative predictive value and accuracy of DTPA-99mTc
scintigraphy for the diagnosis of ATN, AR and CN are displayed in Table-3.
The overall accuracy of scintigraphy for the most important and severe
complications was high (87% for AR, 95% for ATN and 100% for CN) with
good specificity (86% for AR, 89% for ATN and 100% for CN).
DISCUSSION
Acute
or chronic rejection is a main concern in the follow-up of transplanted
patients since it can lead to graft dysfunction and loss. Most methods
used in the evaluation of graft complications are aimed at the early diagnosis
of rejection. The most frequently available non-invasive methods are serial
serum creatinine levels, creatinine clearance, ultrasound (with or without
Doppler scanning), renal scintigraphy (mainly with 99mTc-DTPA
and 99mTc-MAG3), magnetic resonance imaging, urinary cytology,
and serum and immunologic markers. Invasive procedures include intrarenal
manometry, fine-needle aspiration biopsy (FNAB) and core biopsy, considered
the definitive procedure for precise characterization of graft complications.
Accurate non-invasive diagnostic methods
at a lower cost are the preferred techniques to be used. Delaney et al.
(14) compared FNAB, Doppler ultrasound and radionuclide scintigraphy for
the detection of renal graft complications and also performed a cost analysis.
Scintigraphy was the most sensitive method for detection of acute rejection
(70% overall), while FNAB and Doppler ultrasound had sensitivities as
low as 52% and 43%, respectively. The cost of radionuclide scintigraphy
was not considered ideal (only 9% lower than core biopsy). In their study,
FNAB not only had a low sensitivity, but also was insufficient for diagnosis
of renal graft complications in approximately 13% of cases.
Hall et al. (15) also compared radionuclide
scintigraphy and ultrasound without Doppler to biopsy findings, including
the severity of cell infiltration. When performed within 48 hours of biopsy
with heavy mononuclear interstitial cell infiltration, radionuclide scintigraphy
had a sensitivity of 96% for the detection of acute rejection while the
sensitivity of ultrasound was only 21%. Nevertheless, the specificity
of scintigraphy was low, 54%. Sensitivity of radionuclide scintigraphy
was low in cases with mild or no interstitial cell infiltration, but was
still better than that of ultrasound (6/13 patients versus 0/4 patients,
respectively). The radionuclide scintigraphy study frequently contributed
to the final diagnosis particularly when the biopsy findings were inconclusive
or the patient responded to therapy, consistent with the radionuclide
scintigraphy findings. Consequently, the final diagnosis was not always
“independent” of the radionuclide scintigraphy results. In
their experience, a biopsy finding with heavy cellular infiltration was
the most reliable independent factor for the diagnosis of acute rejection.
Akhtar et al. (16) also reported low sensitivity
and specificity of ultrasound and Doppler ultrasound. They found that
an increase in the resistivity index greater than 0.7 was present in 31.5%
of AR but was also elevated in 26.7% of CyT and in 44.4% of ATN. Aktas
et al. (17) reported Doppler ultrasound sensitivities as low as 45% for
low-grade rejections (based on Banff criteria) and as high as 88% for
high-grade rejections. Surprisingly, the same sensitivities were found
for radionuclide scintigraphy when altered perfusion alone was considered.
When the analysis included also altered concentration and retention of
the radiopharmaceutical, sensitivity of scintigraphy increased to 64%
and 100% for low and high grade rejection, respectively, which is still
lower than in other reports.
The most frequent complications found in
the present study (ATN, AR and CN) were those expected to occur in the
early acute phase post transplant, when this population was analyzed (first
3 weeks after surgery).
Radionuclide scintigraphy failed to detect
acute rejection in 6 of the 76 studies (8%). On the other hand, in 3 patients
in whom radionuclide scintigraphy showed AR with negative biopsies, the
clinical follow-up confirmed rejection by improvement in renal function
after systemic treatment with immunosuppressive drugs or new biopsies
performed a few days later. False-negative biopsies can occur, since the
fragment removed may not always be representative of the entire histopathological
process and AR most commonly happens in multiple focal areas. The overall
accuracy of core biopsy has been reported to be about 91% (18,19).
If the false-positive cases of AR were compared
to clinical outcome instead of biopsy results, the specificity and accuracy
of radionuclide scintigraphy for the diagnosis of AR in the current study
would increase to 96% and 91%, respectively.
Detection of ATN was also efficient in the
present group of patients (98%), coupled with a specificity of 95%. Cófan
et al. (20) assessed the value of dynamic radionuclide scintigraphy for
the detection of ATN with 99mTc-MAG3 compared to Doppler ultrasound
in 45 patients with ATN. The authors concluded that Doppler ultrasound
does not discriminate the ATN severity and a resistivity index = 1 in
the baseline study could not be related to a worse prognosis. Nevertheless,
severe ATN was associated with prolonged dialysis treatment and reduced
graft survival.
Although the number of cortical necrosis
events was small (4 cases) in the present study, the high accuracy achieved
was expected to happen, since the alteration in flow and function of the
graft is dramatic. In the present study there was only a single case of
CyT, thus, it was not possible to estimate a reasonable value for the
diagnostic accuracy of radionuclide scintigraphy for the diagnosis of
this complication and CyT is typically a late complication of the transplant.
The high values of sensitivity, specificity
and overall accuracy for the most frequent early graft complications in
this series of renal transplants can be explained because all the patients
analyzed had a previous scintigraphy study in the first 24 hours post
surgery (baseline study), and also because the nuclear medicine physicians
were not blind to the clinical data and that a baseline study is routinely
performed, preferably in the first post operative day, for comparison.
Khajehmugehi et al. (18) concluded after
reviewing 230 episodes of AR in renal transplant recipients, that although
the most sensitive (91%) way to diagnose AR was kidney biopsy, “the
best mode of diagnosing rejection was DTPA isotope scanning.” However,
only the kidney biopsy can give the diagnosis and severity of the acute
rejection, especially in cases when ATN is associated with rejection or
in presence of a vascular component of rejection.
CONCLUSIONS
99mTc-DTPA
scintigraphy is a safe, noninvasive and easy-to-perform method that has
shown a good correlation with biopsy results and clinical evolution of
renal transplanted patients.
We have a strong belief that the best approach
in clinical practice to aid in the correct diagnosis of graft complications
is to routinely perform a baseline 99mTc-DTPA study as screening,
preferably in the first post transplant hours, which is useful for further
comparison, improving the accuracy of this method. Gathering all these
data and using biopsy to confirm diagnosis, leads to prompt intervention
when necessary.
The early detection of severe graft complications
such as rejection, vascular thrombosis or graft necrosis will lead to
their prompt treatment, reducing the risks of further kidney damage or
of complications derived from the presence of a non-viable graft.
REFERENCES
- Kirchner PT, Rosenthall L: Renal transplant evaluation. Semin Nucl Med. 1982; 12: 370-8.
- Lubin E, Shapira Z, Melloul M, Youssim A: Scintigraphic detection of vascular and urological complications in the transplanted kidney: 133 cases. Eur J Nucl Med. 1985; 10: 313-6.
- Rutland MD: A comprehensive analysis of renal DTPA studies II: Renal transplant evaluation. Nucl Med Commun. 1985; 6: 21-30.
- Dubovsky EV, Russell CD, Bischof-Delaloye A, Bubeck B, Chaiwatanarat T, Hilson AJ, et al.: Report of the Radionuclides in Nephrourology Committee for evaluation of transplanted kidney (review of techniques). Semin Nucl Med. 1999; 29: 175-88.
- Isiklar I, Aktas A, Uzuner O, Demirag A, Haberal M: Power Doppler ultrasonography compared with scintigraphy in the diagnosis of renal allograft dysfunction. Transplant Proc. 1999; 31: 3330-1.
- Neimatallah MA, Dong Q, Schoenberg SO, Cho KJ, Prince MR: Magnetic resonance imaging in renal transplantation. J Magn Reson Imaging. 1999; 10: 357-68.
- Brown ED, Chen MY, Wolfman NT, Ott DJ, Watson NE Jr.: Complications of renal transplantation: evaluation with US and radionuclide imaging. Radiographics. 2000; 20: 607-22.
- Heaf JG, Iversen J: Uses and limitations of renal scintigraphy in renal transplantation monitoring. Eur J Nucl Med. 2000; 27: 871-9.
- George EA, Codd JE, Newton WT, Haibach H, Donati RM: Comparative evaluation of renal transplant rejection with radioiodinated fibrinogen, 99mTc-sulfur colloid, and 67Ga-citrate. J Nucl Med. 1976; 17: 175-80.
- Carmody E, Greene A, Brennan P, Donohue J, Carmody M, Keeling F: Sequential Tc-99m mercaptoacetyl-triglycine (MAG3) renography as an evaluator of early renal transplant function. Clin Transplant. 1993; 7: 245-9.
- Oriuchi N, Miyamoto K, Hoshino K, Imai J, Takahashi Y, Sakai S, et al.: 99mTc-MAG3: a sensitive indicator for evaluating perfusion and rejection of renal transplants. Nucl Med Commun. 1997; 18: 400-4.
- el Maghraby TA, van Eck-Smit BL, de Fijter JW, Pauwels EK: Quantitative scintigraphic parameters for the assessment of renal transplant patients. Eur J Radiol. 1998; 28: 256-69.
- Racusen LC, Solez K, Colvin RB, Bonsib SM, Castro MC, Cavallo T, et al.: The Banff 97 working classification of renal allograft pathology. Kidney Int. 1999; 55: 713-23.
- Delaney V, Ling BN, Campbell WG, Bourke JE, Fekete PS, O’Brien DP 3rd, et al.: Comparison of fine-needle aspiration biopsy, Doppler ultrasound, and radionuclide scintigraphy in the diagnosis of acute allograft dysfunction in renal transplant recipients: sensitivity, specificity, and cost analysis. Nephron. 1993; 63: 263-72.
- Hall JT, Kim EE, Pjura GA, Maklad NF, Sandler CM, Verani R: Correlation of radionuclide and ultrasound studies with biopsy findings for diagnosis of renal transplant rejection. Urology. 1988; 32: 172-9.
- Akhtar F, Rana TA, Kazi J, Zafar N, Hashmi A, Bhatti S, et al.: Correlation between biopsies and noninvasive assessment of acute graft dysfunction. Transplant Proc. 1998; 30: 3069.
- Aktas A, Isiklar I, Gulaldi NC, Dermirag A, Demirhan B: Sensitivity of radionuclide imaging, Doppler, and gray-scale ultrasound to detect acute rejection episodes, based on the pathologic grade of acute rejection. Transplant Proc.1998; 30: 786-7.
- Khajehmugehi AR, Mehrsai AR, Taheri M, Khan ZH: Evaluation of acute kidney rejection in 230 renal transplant recipients. Transplant Proc. 1998; 30: 730-1.
- Hughes D: Fine-Needle Aspiration Cytology of the Transplanted Kidney, In: Morris PJ (ed.). Kidney Transplantation. 5th Ed. Philadelphia, PA, WB Saunders. 2001, 392-407.
- Cófan F, Gilabert R, Oppenheimer F, Bru C, Lomena F, Setoain F, et al.: Dupplex-Doppler ultrasound and MAG-3 scintigraphy in the evaluation of acute tubular necrosis after kidney transplantation. Transplant Proc. 1997; 29: 1376-7.
____________________
Received:
July 21, 2003
Accepted after revision: November 14, 2003
_______________________
Correspondence address:
Dr. Elba C.S.C. Etchebehere
Serviço de Medicina Nuclear, Depart Radiologia
Hospital das Clínicas da UNICAMP
Caixa Postal 6142, Campinas, 13081-970, Brazil
Fax: + 55 19 3251–1041
E-mail: elba@mn-d.com