TECHNIQUE
OF KIDNEY TRANSPLANTATION IN MICE WITH ANTI-REFLUX URINARY RECONSTRUCTION
(
Download pdf )
PAULO N. MARTINS
Department of Surgery, Division of Transplant Surgery, Brigham and Women’s Hospital, Harvard Medical School, Boston, MA, USA
ABSTRACT
Experimental models of organ transplantation play a crucial role in establishing the principles of transplantation immunobiology. Murine transplant models of vascularized organs are particularly useful for immunobiological studies because there are more immunological tools available. However, the technique of kidney transplant in mice is very challenging. A difficult aspect of this model is urinary reconstruction, which is frequently associated to complications. In this article, the technique of mouse kidney transplantation using an anti-reflux system (modified extravesical ureteroneocystostomy) is described and illustrated for the first time. Although technically demanding, this procedure is feasible and may reduce the incidence of urine leakage and reflux.
Key
words: kidney transplantation; experimental model; mouse; microsurgery
Int Braz J Urol. 2006; 32: 713-20
INTRODUCTION
Transplant
models of vascularized organs in the mouse are particularly useful for
immunobiological studies because there are more immunological tools available
(inbred, transgenic and knockout animals; genetic mapping, monoclonal
antibodies, reagents, etc.) (1,2).
The technique of mouse kidney transplantation
was first established by Skoskiewicz & Russel already in 1973 (3),
then improved by Kalina (4) and Zhang (5). However, it is currently performed
only in a few transplantation centers in the world, due to the anastomoses
complexity (renal artery diameter 0.3 mm).
SURGICAL TECHNIQUE
Male
inbred C57BL/6 mice (Jackson Laboratories) weighting 20-30 g were used
for kidney transplantations. Animals were housed and cared for in accordance
with our institution’s guidelines for experimental animals. In a
small series of 20 animals, consecutively operated using this technique,
the failure rate was 50% and apparently related to vascular complications.
Mice were anesthetized with a solution of
ketamine (80 mg/kg i.p.) and xylazine (5 mg/kg i.p.) mixed in a normal
saline solution. All procedures were performed at 4-25x magnification
using a microscope (SMZ800, Nikon, Japan) and standard microsurgical instruments.
Donor Operation
After induction of anesthesia, the mouse
was shaved, fixed on the operating board and the abdomen was prepped with
betadine. To assure normal volemia, a saline solution was instilled in
the abdominal cavity whenever it became dry. A midline incision from the
xyphoid appendix to pubis was performed and exposure was achieved using
small retractors to keep liver and bowels away from the left kidney.
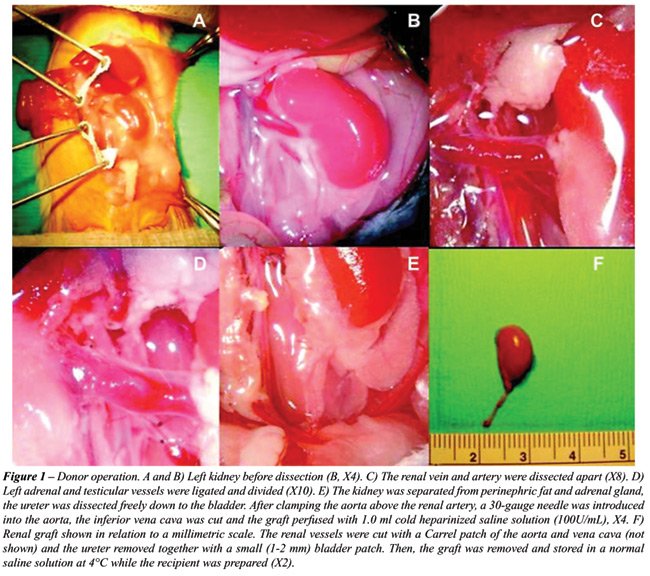
The renal vein and artery were dissected
apart under X20 magnification avoiding direct manipulation of the vessels.
Left adrenal and testicular vessels were ligated with 10-0 polypropylene
sutures and divided. Then, the kidney was separated from the perinephric
fat and adrenal gland, the ureter was dissected freely down to the bladder
without stripping its fat and cut with a small (1-2 mm) bladder patch.
After clamping the aorta above the renal artery, a 30-gauge needle was
introduced into the aorta, the inferior (caudal) vena cava was cut and
the graft perfused with 1.0 mL cold heparinized saline solution (100U/mL).
Renal vessels were cut with a Carrel patch of the aorta and vena cava
and the graft was removed and stored in a normal saline solution at 4°C
for 20 min. until the time of transplantation (Figure-1).
Recipient
Operation
To increase the success rate, a two-stage
procedure was performed, i.e. the left native kidney was removed at the
time of grafting and the right native kidney was left in place until day
7, when the right nephrectomy was performed.
A midline incision from the xyphoid appendix
to pubis was performed, and exposure was achieved using small retractors
to keep liver and bowels away from the kidney. The renal pedicle was ligated
with 7-0 silk suture and the recipient left kidney was removed leaving
place for the donor kidney.
After ligating some lumbar branches, the
infrarenal aorta and inferior vena cava were isolated and two loops of
7-0 silk were placed proximally and distally around them and tied to promote
homeostasis. Elliptical longitudinal aortotomy and cavotomy were performed
between these ties and the vessels were flushed to clear blood inside
them. Vascular anastomoses were performed end-to-side to the abdominal
aorta and vena cava using a running 11-0 nylon suture (Ethilon, Ethicon,
USA). To anastomose the renal artery, two stay sutures (11-0 nylon suture)
were placed at the artery’s opposite ends (inferiorly and superiorly).
The back wall was sewn first, through a transluminal approach; then the
anterior wall, both with a continuous suture. In general, only four to
five stitches on each side are necessary to avoid bleeding.
The vein was anastomosed in the same fashion
as the artery. Before suturing the vein, it is important to confirm it
is not twisted. Depending on the size of the caval patch, 5 to 7 times
the vein was stitched on each side, avoiding pinching the opposite wall.
After both anastomoses were performed, the first distal loop was loosened
and then the proximal loop. Blood flowed back into the kidney and bleeding
was minimal. Saline was usually given subcutaneously proportional to the
bleeding (Figure-2).

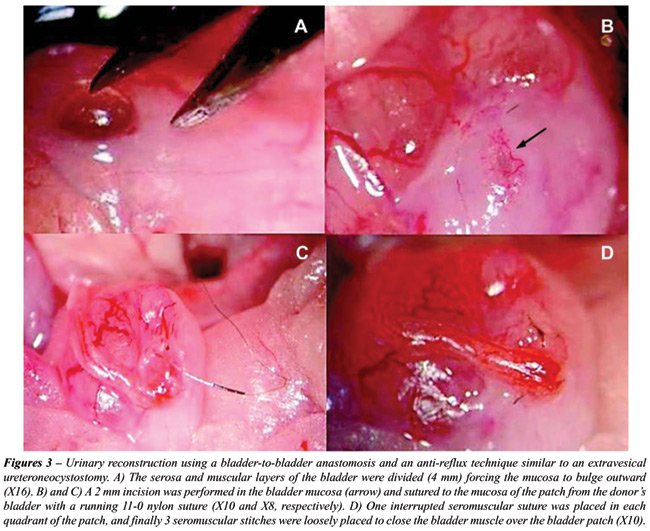
Urinary reconstruction was established by
suturing the small bladder patch to a cystotomy located on the bladder
dome (similar to the Lich-Gregoir technique for extravesical ureteroneocystostomy).
The animal should be well hydrated to keep the bladder filled. First,
the serosa and muscular layers of the posterolateral aspect of the bladder
were divided (5 mm) with the micro-scissors avoiding major vessels and
taking care not to enter the bladder. This develops a plane between the
muscularis and mucosa allowing the mucosa to bulge out. Then, the bladder
mucosa was divided (2 mm) and sutured to the mucosa of the patch from
the donor’s bladder with a running 11-0 nylon suture (Ethilon, Ethicon,
USA). Then, one interrupted seromuscular suture was placed in each quadrant
of the patch, and finally three interrupted 11-0 nylon seromuscular sutures
were loosely placed over the patch to close the bladder muscle over the
bladder patch and terminal ureter, burying the anastomosis, sealing the
first suture and creating a muscular tunnel to reduce the risk of urine
reflux (Figure-3).
Abdominal wall and skin were closed with
a continuous 5-0 absorbable suture (Vycryl, Ethicon, USA). A saline 0.5
mL solution was given subcutaneously after the transplant and no antibiotics
or heparin were given. Mice were kept under a heating lamp until they
were awake.
COMMENTS
Mouse
kidney transplantation is a very demanding microsurgical procedure full
of details, which requires long training and meticulous technique. The
murine kidney is extremely sensitive to ischemia/reperfusion injury, and
to perform a successful operation the time of anastomosis (warm ischemia)
should be less than 35 minutes. Most experiments show that in experienced
hands the survival rate is between 40 and 70% (3,4). The learning curve
is slow because the risk of renal artery thrombosis is very high and difficult
to avoid, and due to urological complications.
In rat kidney transplantation, continuity
of urine flow is reestablished most commonly by end-to-end ureter-ureter
anastomosis (splinted or non-splinted). On the other hand, kidney transplantation
in mice, probably because of the very small diameter of the ureter, ureter-to-ureter
anastomosis has not been described. In the literature, urinary reconstruction
in mouse kidney transplantation has been performed either by direct implantation
of the ureter in the bladder without anastomosis or most commonly by bladder-to-bladder
anastomosis using a large bladder patch. The blood supply of the terminal
ureter and bladder patch is exclusive from the graft vasculature and prone
to ischemia. Not uncommon, the use of a large bladder patch is associated
with either bladder necrosis and urine leakage or neurogenic bladder with
calculi formation due to bladder denervation (6).
The most preferred technique for urinary
reconstruction in clinical kidney transplantation is extravesical ureteroneocystostomy.
Differently from the technique of extravesical ureteroneocystostomy used
in the clinic, the author opted for using a small bladder patch since
spatulation of the mouse ureter would be difficult. No splint was used
since it has been associated with more urological complications (6), and
the bladder patch allows enough area to place sutures. The technique described
here avoids continuous (running) suture of muscular layer that increases
ischemia and the risk of patch necrosis and urine leakage. Water-tightness
is ensured by minimal vesical opening and continuous suture. The incidence
of vesical calculi depends also on the suture material used for urinary
reconstruction (6), and therefore, newer absorbable microsutures are preferred.
An anti-reflux system, although time-consuming
and difficult to perform, may reduce the incidence of urosepsis related
to urinary fistulae and reduce the risks of hydronephrosis and chronic
pyelonephritis in the long-term. To the author’s knowledge this
is the first report on urinary reconstruction in the mouse using an anti-reflux
technique. The potential advantages of this technique applied in the murine
model still need to be confirmed in the long-term in case-control studies.
ACKNOWLEDGEMENT
This work was performed at the Charité-University Medicine Berlin, Virchow Clinic, Department of General Surgery and Transplantation, Berlin, Germany.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Martins PN: Importance of microsurgery for organ transplantation. Acta Cir. Bras. 2003; 18: 59-61.
- Martins PN, Filatenkov A: Microsurgical techniques for experimental kidney transplantation and general guidelines to establish studies about transplantation immunology. Acta Cir Bras. 2003; 18: 355-60.
- Skoskiewicz M, Chase C, Winn HJ, Russell PS: Kidney transplants between mice of graded immunogenetic diversity. Transplant Proc. 1973: 721-5.
- Kalina SL, Mottram PL: A microsurgical technique for renal transplantation in mice. Aust N Z J Surg. 1993; 63: 213-6.
- Zhang Z, Schlachta C, Duff J, Stiller C, Grant D, Zhong R: Improved techniques for kidney transplantation in mice. Microsurgery. 1995; 16: 103-9.
- D’Silva M, Gittes RF, Wolf P, Pirenne J, Munger K, Pascual J, et al.: Rat kidney transplantation update with special reference to vesical calculi. Microsurgery. 1990; 11: 169-76.
____________________
Accepted
after revision:
August 9, 2006
_______________________
Correspondence address:
Dr. Paulo Ney Aguiar Martins
Division of Transplant Surgery
Brigham and Women’s Hospital
221 Longwood Ave, Rm 309
Boston, Massachusetts, 02115, USA
Fax: + 1 617 732-5724
E-mail: pmartins@partners.org
EDITORIAL COMMENT
Clinical kidney transplantation has become the preferred method of renal replacement therapy worldwide. Testing new pharmacological and biological agents, and identifying new methods to diagnose and treat rejection depends on preclinical investigation. The use of large animal models such as the monkey, dog, cat, pig, etc. in transplant research has become problematic due to high cost, the need for specialized animal care, longer gestation and life spans, and cultural sensitivities regarding certain species. Therefore, the rodent is usually preferred. The rat is of sufficient size (300-400 grams) to permit solid organ transplant experiments using microsurgical techniques, but has been less well characterized than the mouse in molecular biology. Since much of the focus on molecular immunology and genetics has been targeted to murine models (monoclonal antibody production, transgenics, knock in and knock out recombinations, etc.), the mouse is better suited to transplant experimentation. However, the adult mouse (30-50 grams) is 5-10 times smaller than the rat, more difficult to perform microsurgery, and ultimately more prone to technical failures. A major limiting factor in murine whole organ kidney transplantation has been the ureteral reconstruction. The author offers a nice technique of simplifying the anastomosis of the small ureter by using a donor bladder patch. This technique, similar to the human extravesical ureteral anastomosis, may also limit post transplant urinary infections by creating an anti-reflux tunnel. Any approach that simplifies microsurgical transplant techniques in murine models would be a welcome addition to this difficult endeavor. This technique should be tried by other murine microsurgical teams to see if diminished technical failures can reinvigorate the wider use of murine kidney transplants for long term models.
Dr. Stuart
M. Flechner
Director, Clinical Research
Section of Renal Transplantation
Cleveland Clinic Foundation
Cleveland, Ohio, USA
E-mail: flechns@ccf.org
EDITORIAL COMMENT
The
author reports for the first time a modified extravesical ureterocystoneostomy
for urinary tract reconstruction in the mouse kidney transplant model.
After completion of the vascular anastomosis the bladder dome is incised
over a length of 5 mm avoiding cutting into the mucosa. The mucosa is
opened at the distal end of the submucosal tunnel over a distance of approximately
2 mm. The transplant ureter together with its distal end and a small bladder
patch is then anastomosed to the mucosa. Thereafter, the muscularis of
the bladder wall is readapted over the implanted transplant ureter with
3 interrupted sutures.
Since
the first description by Fisher & Lee, the use of rat-inbred strains
as an investigational model of renal transplantation has been extensively
used (1). Microsurgical techniques have been developed to the extent that
the postoperative survival of renal grafted rats is now routine. However,
renal transplantation in mice is technically very demanding due to the
small vessels size and the inherent risk of vascular thrombosis and graft
loss. Furthermore, reconstruction of the urinary tract has been associated
with upper urinary tract obstruction as well as ureter and bladder patch
necrosis (2). The learning curve in kidney transplantation in mice is
substantially longer than in rats and the mortality rate, as stated by
the author, is as high as 50%, even in the hands of experienced microsurgeons
and long-term survival rates are sparse. A survival rate of more than
4 weeks has been reported by the same author in only 4 animals (8%) in
a consecutive series of 50 kidney transplant procedures in mice using
a bladder to bladder patch for urinary tract reconstruction (3). Most
animals died due to surgical related complications.
Therefore,
it seems of utmost importance to balance the advantages and disadvantages
of performing a technical demanding antireflux procedure during kidney
transplantation in mice. Prolonged surgical time in small animals, as
for performing an extravesical ureterocystoneostomy, may lead to hypothermia
and eventually death and has to be considered as a major risk factor (4).
Further, performing an antireflux procedure does not inevitably allow
drawing the conclusion that there is no vesicoureteral reflux and that
the graft is protected against the possibility of upper urinary tract
infection. In humans the key to success to prevent vesicoureteral reflux
according to Grégoir is to create a submucosal tunnel of 5 to 6
cm length (5). However, it remains to be determined how long the submucosal
tunnel has to be in mice to prevent vesicoureteral reflux.
REFERENCES
- Fisher B, Lee S: Microvascular surgical techniques in research, with special references to renal transplantation in the rat. Surgery. 1965; 58: 904-14.
- Russell PS, Chase CM, Colvin RB, Plate MD: Kidney transplantation in mice: an analysis of the immune status of mice bearing long-term, H-2 incompatible transplants. J Exp Med. 1978; 22: 1449-68.
- Martins PN: Learning curve, surgical results and operative complications for kidney transplantation in mice. Microsurgery. 2006 (ahead of print).
- Pahlavan PS, Smallegange C, Adams MA, Schumacher M: Kidney transplantation in rats: assessments, complications and management. Microsurgery. 2006; 26: 404-11.
- Grégoir W: The surgical treatment of congenital vesico-ureteral reflux. Acta Chir Belg. 1964; 63: 431-9.
Dr. Martin Schumacher
FMH Urologie, FEBU
Urologkliniken
Karolinska University Hospital
SE-171 76 Stockholm, Sweden
E-mail: Martin.Schumacher@insel.ch