VIDEOENDOSCOPIC
SURGERY BY EXTRAPERITONEAL ACCESS: TECHNICAL ASPECTS AND INDICATION
(
Download pdf )
M. TOBIAS-MACHADO, ROBERTO V. JULIANO, HELOISA A. GASPAR, RICARDO P. ROCHA, MILTON BORRELLI, ERIC R. WROCLAWSKI
Discipline of Urology, ABC School of Medicine (FMABC), Santo André, São Paulo, Brazil
ABSTRACT
Laparoscopic
surgery in urology is definitely incorporated to the techniques of minimally
invasive treatment for urogenital diseases. Though the classic access
to organs in the urinary tract is extraperitoneal, this access has not
been prioritized when the videoendoscopic technique is used. In Brazil,
few groups use this approach and little has been discussed about its true
practical applicability.
The authors intended to discuss the main
technical aspects and criteria for indication, reported though the improvement
achieved in a 5-year period with 150 operated cases.
A review of the literature shows that the
worldly acceptance of the extraperitoneal endoscopic approach is increasing.
Nevertheless, there are no evidences that the extraperitoneal access is
superior to the transperitoneal route. Thus, the choice depends basically
on the surgeon’s preference. Major advantages are the immediate
access to the renal hilum and isolation of peritoneal structures. Employing
this access is useful when one suspects that significant peritoneal adherences
could prevent the surgical act or when one wishes to preserve the integrity
of the peritoneal cavity.
Key
words: video-assisted surgery; laparoscopic surgery; retroperitoneal
space
Int Braz J Urol. 2003; 29: 441-9
INTRODUCTION
Ablative
laparoscopic surgery in urology is widely accepted in selected situations
because it presents well defined advantages in relation to open surgery,
such as earlier return to routine activities, reduction in the hospitalization,
decreased blood loss and reduction in analgesic use post-operatively,
in addition to superior esthetic result (1,2).
Extraperitoneal access is the preferential
route in cases of open urologic surgery because it provides a direct approach
to the organs of the urinary system, without the need of manipulating
the bowel, with a lower possibility of paralytic ileus and with drainage
of the open urinary tract without contact with the peritoneal cavity.
Despite these features, few specialized centers have prioritized the retroperitoneal
approach when videoendoscopic access is employed.
Most authors give preference to the transperitoneal
route due to the “larger working space” and greater facility
in viewing anatomical structures, what would result in a lower learning
curve, especially for those who are initiating in laparoscopy (1,3).
The first report of therapeutic retroperitoneoscopic
access in urology dates from 1978, when Wickham (4) performed the extraction
of a proximal ureteral stone. However, proper standardization and popularization
of the technique were established by Gaur in 1992, with the development
of the atraumatic balloon for retroperitoneum expansion (5). Since then,
some groups in the United States, France, Germany and Japan have published
their results relative to this technique (6-8). In our setting, we have
used, preferably, this access, since 1997, in the treatment of several
urologic diseases (3).
We intended to describe the technical aspects
and main advantages and disadvantages of this minimally invasive access,
comparing them to data in the literature.
SURGICAL TECHNIQUE AND STRATEGY
General
Checking of Material – The material required for surgery is the same used for conventional laparoscopic surgery, added by some details that are inherent to each particular surgical procedure.
Disposition
in the Surgical Room – In lumbar access, the surgeon operates
the patient in a position similar to open surgery, that is, posterior.
Due to the lateral position of the patient in the surgical table and the
long length of the laparoscopic material, we recommend that the surgeon,
for better comfort, be positioned over an estrade. The camera stands beside
the surgeon with the assistant and the instrumental table, at the contralateral
side (Figure-1).
The positioning of the surgical team for
pelvic surgery is the same described for transperitoneal laparoscopic
surgery (Figure-2).
Lumbar Surgery
Position of the Patient – The patient is placed in lateral decubitus, opposed to the side intended for surgery, the table is flexed in order to raise the flank area and to enlarge the space between the iliac crest and the costal border. The patient is fixed in this position and the extremities are arranged in order to avoid or minimize neuromuscular sequelae.
Access to the Retroperitoneum - The retroperitoneal cavity must to be created in order to position the trocars and develop the surgical procedure. Initially a transverse incision is performed by 1.5 cm planes, below the extremity of the 12th rib the thoracolumbalis fascia is opened, reaching the retroperitoneal space. A careful digital dissection is performed in the anterior, postero-superior and inferior directions, promoting the separation between the psoas muscle posteriorly and the Gerota’s fascia anteriorly (9). It is important to ensure that all entrance ports are largely free of adherences, so that punctures can be performed under direct viewing, without lesion of adjacent organs.
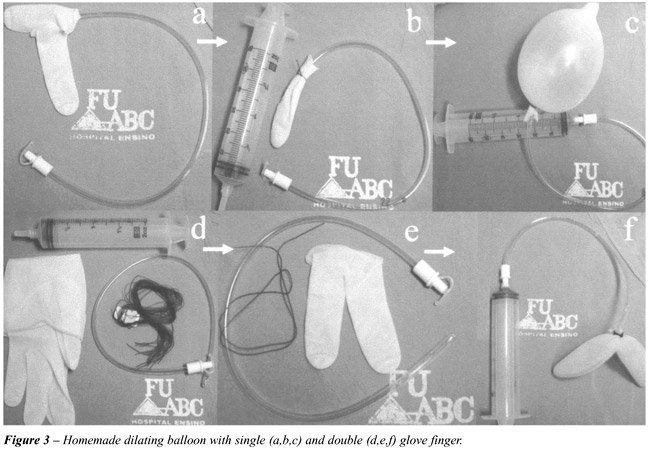
Introduction
of the Atraumatic Balloon – There is some controversy in the
literature relative to the need of using a balloon for retroperitoneum
dilatation. There are commercially available products, such as the balloon
trocar, that make this access easier, where the space can be created under
optical viewing inside the balloon, monitoring the dissection. In order
to optimize costs, some authors have adapted expansion systems with lower
cost materials (8,10-12). We have used a balloon made through a double
glove finger (placing one finger inside the other so to obtain greater
resistance against rupture), tied with a cotton thread to a 18F urethral
catheter, where we inject physiologic saline solution. This device allows
a 500 - 1000 mL capacity, depending on the procedure to be performed (Figure-3).
In procedures where we intend to approach the middle/distal ureter (especially
nephroureterectomies), we use the 2 balloons technique previously described
by Gill et al. (13).
Initially, as preconized by Gaur, we left
the balloon inflated for 10 minutes, with the objective of performing
the hemostasis of small vessels. Based on the experience of certain groups
that perform only the digital technique, we started to remove the balloon
immediately after its expansion and we did not observe bleeding or any
difference in the quality of the images obtained.
Creation
of Pneumoretroperitoneum - A Hasson trocar (10-12 mm) is introduced
under direct viewing into the incision and fixed with 2-0 cotton sutures,
in order to avoid escape of air (Figure-4). There are special devices
such as the threaded trocar (Figure-4B) or with inflatable balloon (Figure-5)
that allow an excellent sealing, however with higher costs. When a Hasson
trocar is not available, it is possible to employ muscular purse-string
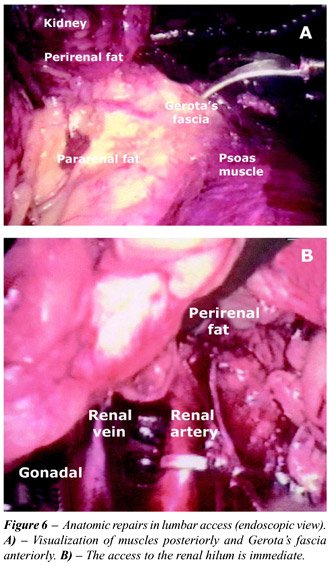
suture and a common trocar for such function. The retroperitoneum is insufflated
with carbon dioxide through this trocar until a pressure of 15 mmHg is
reached. A laparoscope of 0° or 30° is introduced into this port,
enabling the viewing of the musculature posteriorly, and the Gerota’s
fascia and peritoneum anteriorly (Figure-6). We have worked with a 0°
optics. The 30° optics can be especially useful during the dissection
of the kidney’s superior pole and adrenal glands, which are places
located deeper and with difficult access under linear viewing.

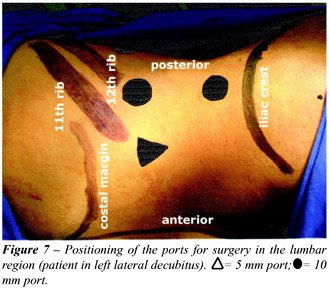
Secondary
Ports – All of them are introduced under direct viewing with
the aid of optics. The second port (10 mm) is positioned 2 cm above the
iliac crest, through the floor of the inferior lumbar triangle (Petit).
Some authors prefer to start the retroperitoneal access at this point.
Next, the optics is transferred to this port. The third port (5 mm) is
placed 1.5 cm inferior and lateral to the angle formed between the lower
edge of the 12th rib and the paravertebral muscles, making sure that it
penetrates above the subcostal nerve. This port and the access port are
used by the surgeon. The fourth port (5 mm) is manipulated by the assistant
in order to separate the structures and must be introduced below the extremity
of the 11th rib or in medial position in the anterior axillary line so
that it does nor perforate the peritoneum (Figure-7) (14).
Slight variations are required according
to the procedure. For adrenal surgery, punctures are made at a 1-2 cm
more anterior position, to make the access to the gland easier, especially
the most posterior trocar, which could present difficulty during the approach
in a conventional position due to the distance and the limitation in the
forceps length.
The same access is useful when one intends
to perform sutures, allowing a better approach angle to the renal pelvis
(pyeloplasty and pyelolithotomy). In such cases a slight lateral decubitus
to the surgeon side is necessary in order to promote better comfort.
Still on access variations, it can be useful
to replace the assistant’s 5 mm trocar by a 10 mm trocar in cases
there it is necessary to separate more widely the peritoneum (giving access
to a liver retractor), such as in adrenal surgeries or when a peritoneal
perforation occurs, rendering the procedure difficult.
When the surgeon intends to perform a nephroureterectomy,
the port of the Petit’s triangle is placed in a more anterior position,
so that it enables a better distal view of the ureter, and the surgeon
can perform urethral dissection moving to the other side and using a more
medial and more inferior puncture, with the optics being transferred to
superior median puncture. In this situation, the change in the spatial
orientation requires the monitor to be transferred to the patient’s
lower region.
Pelvic Surgery
Position of the Patient – The patient is placed in semi-gynecologic position with a Foley’s catheter draining the bladder. We prefer using a wooden plate in the shape of an inverted “Y”, but it is possible to adapt the position in a table with stirrups. When the approach over the bladder or the urethra is nor necessary (lymphadenectomy), the patient can be placed in supine position.
Approach
to the Pre-Peritoneal Region – A 1.5 cm arcuate incision in
the umbilicus or a vertical intra-umbilical incision is made. The dissection
is performed in the subcutaneous tissue and the aponeurosis, promoting
its transverse opening, close to the linea alba. It is possible to view
the Douglas’ arcuate line posteriorly and the borders of the abdominal
rectus muscle laterally. The medial region of the abdominal rectus muscle
is digitally dissected towards the Retzius’ space and until the
pubic symphysis, moving the peritoneum posteriorly.
Similar to the lumbar access, all the potential
entrance sites for the trocar must be released from the peritoneum, in
order to avoid its perforation. Sites that are more difficult to dissect
are the lateral regions of hypogastrium (lateral insertion of the Douglas’
ligament). Differently from the transperitoneal access, a largely exaggerated
Trendelemburg position is not necessary, since the intact peritoneum provides
support to the bowel, a fact that can promote anesthetic advantages resulting
from a smaller cephalic slope.
Introduction of the Atraumatic Balloon – The dilating balloon is positioned in the Retzius’ space and insufflated with 800-1000 mL of saline solution distending the extraperitoneal region. For procedures where we don not need a larger dissection of the median plane (lymphadenectomy or Burch surgery), we idealized a balloon with 2 simultaneous glove fingers that would have the advantage of expanding more efficaciously the lateral regions (sites with a more difficult access to digital dissection) (Figure-4).
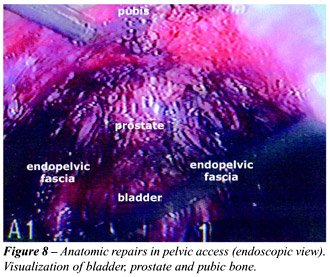
Creation
of Pneumoretroperitoneum – Performed similarly to the lumbar
access. Upon verifying the created space, it is possible to view the bladder,
the pubic symphysis and eventually the iliac vessels (Figure-8).
Secondary
Ports – The number and position of ports depend on the surgical
procedure to be performed (Figure-9). A 10 mm trocar positioned on the
median line 2 cm above the pubic symphysis can be used for the surgeon’s
work, jointly with a forceps that is introduced in the 5 mm trocar, 2
cm superior and medial to the antero-superior iliac spine, opposite to
the side that will be approached. We prefer this conformation for pelvic
lymphadenectomy. Some procedures can be performed with only 3 ports (2
in iliac fossae for the surgeon), as in Burch’s surgery.
Complex procedures such as radical prostatectomy
require 5 ports, 2 of them placed between the optics and the punctures
in iliac fossa (suited for dissection and sutures).

COMMENTS
Extraperitoneal
access represents the preferential approach in conventional urologic surgeries
(13,15,16). However, the initial application of extraperitoneal videoendoscopic
surgery presents greater technical difficulty, mainly due to a smaller
working space, lower lightning and the spatial orientation, which are
responsible for a larger learning curve (6-8). The issue of working space
is relative and directly associated with a good peritoneal detachment
and proper installation of the ports, being feasible even in children
(17,18). Concerning the spatial orientation, the optics must be always
kept in a position where it is possible to observe the posterior muscles
in horizontal position, thus allowing anatomical parameters to be identified.
In our Service, where 150 retroperitoneoscopic procedures were performed
up to now, we did not observe a greater difference in the technical adaptation
for this approach, when compared with the transperitoneal route.
We believe that the expansion of the extraperitoneal
space with the aid of the atraumatic balloon – either hand-made,
industrialized, direct viewing-guided or not – is recommendable
since it enlarges the surgical field in areas that cannot be reached by
the finger, reducing the need of forceps dissection (3,14,17). The use
of the balloon trocar has the advantage of allowing the visualization
of structures, especially the renal pedicle, during the expansion. Most
authors do not believe that the location of the dilating balloon inside
Gerota’s fascia is essential, as it was originally described by
Gaur (5).
The creation of the pneumoretroperitoneum
is similar to the one performed in the transperitoneal access, including
the recommended pressure of 15 mmHg. There is controversy about the repercussions
caused by the pneumoretroperitoneum when compared with pneumoperitoneum.
Some works initially proposed the occurrence of a higher absorption of
CO2 in pneumoretroperitoneum. Currently, it is believed that hypercapnia
produced by CO2 insufflation does not differ between transperitoneal and
retroperitoneal accesses, with rates around 5-10%, and rarely with the
appearance of clinical manifestations (8,19).
There are also reports of a higher index
of pneumothorax with the extraperitoneal lumbar access resulting of pleural
perforations promoted by dissection close to the pleura or by the higher
diffusion of gas to the pleural space. Wolf et al. documented an incidence
of pneumothorax / pneumomediastinum of 41% with no clinical repercussions,
in patients submitted to extraperitoneal laparoscopy (19). Gill et al.
observed the occurrence of pneumothorax and pneumomediastinum in 0.6%
and 0.4%, respectively. Nevertheless, they stress that the post-operative
radiological control was not routinely performed in all patients, and
those values could be underestimated due to undiagnosed subclinical cases
(8).
The permanent surgical material used in
retroperitoneoscopy is similar to that used in conventional laparoscopy,
except for the Hasson trocar, which eventually can be replaced by a common
10 mm trocar fixed to the aponeurosis by a “purse-string”
suture.
Excess or improper location of trocars can
promote a collision between the forceps, a fact known as “trocars
conflict”, responsible also for a greater difficulty in suture.
Due to these issues, few series report reconstructive procedures through
extraperitoneal access (3,7,20).
Inadvertent peritoneal opening, with resulting
pneumoperitoneum, can increase the grade of technical difficulty. It is
more pronounced during pelvic surgeries, since in lumbar surgeries the
lateral position displaces the bowel medially (8). When it is not possible
to proceed with the surgery, a transperitoneal puncture can be made for
escape of air, as well as the conversion to transperitoneal laparoscopic
technique or, as the last option, conversion to open technique.
The bagging of organs in the extraperitoneal
space can also be more laborious, especially when industrialized bags
with a rigid entrance hole are not available. Some authors, in more difficult
cases, suggest the opening of the peritoneum at the end of the procedure
in order to increase the space, making the maneuver easier (6). We have
not used this maneuver routinely, since it is usually possible to handle
the specimen in the retroperitoneal space. When the specimen is too large
and requires the enlargement of one of the ports, we enlarge the incision
and introduce the bag in the retroperitoneum under viewing, favoring the
introduction of the specimen in the surgical bag as well.
There are some factors that can hamper or
prevent the use of extraperitoneal access. The presence of obesity, which
results in a higher amount of retroperitoneal fat, is a factor of increasing
difficulty for identifying structures of the renal pedicle and adrenal
gland. Despite the surgical time getting longer and the surgery being
a lot more laborious, the benefits for this group of patients are indisputable.
Conditions where there is no capacity for
creating a space between the kidney and the abdominal musculature, such
as previous retroperitoneal surgery, severe renal inflammation and the
presence of very large kidneys, are relative contra-indications. In such
situations it is possible to try to create the space and, in case of impossibility,
the access port is used as an adjunct in the transperitoneal approach.
We must also remind that in such cases, surgical difficulties will be
found in the transperitoneal access as well, however with a larger space
for work. Hemal et al. (12) reported the use of laparoscopic nephrectomy
in 18 patients with large hydronephrosis (over 1,000 mL in volume, which
surpassed the middle line or extended themselves by more than five vertebral
spaces), being 12 by retroperitoneal route. Hobart et al. also presented
their favorable experience with bilateral extraperitoneal nephrectomy
for polycystic kidneys (21). Contrary to most laparoscopists, both works
preconize the extraperitoneal access as a choice in the management of
kidneys with large dimensions. Hemal et al. showed also a large experience
in the treatment of renal inflammatory pathologies (including pyonephrosis
and tuberculosis), demonstrating that it is possible to use the extraperitoneal
approach even when local inflammation is predicted (11).
CONCLUSION
The choice of access is fundamentally based in the surgeon’s preference and in particularities in each case. The assumed difficulties that occur with the extraperitoneal access can be resolved if a rigorous technical standardization is achieved. Considering the advantages and limitations previously discussed, we use the extraperitoneal approach as the choice access in the majority of laparoscopic procedures in urology. We believe that even for surgeons who prefer the transperitoneal access, knowing the extraperitoneal access is useful, since it can be needed in patients with antecedents of major abdominal surgery or previous peritonitis, situations where intraperitoneal adhesions can hinder the transperitoneal surgery.
REFERENCES
- Abbou CC, Cicco A, Gaswan D: Retroperitoneal laparoscopic versus open radical nephrectomy. J Urol.1999; 161: 1776-80.
- Winfield HN, Hamilton BD, Bravo EL, Novick AC: Laparoscopic adrenalectomy: the preferred choice? A comparison to open adrenalectomy. J Urol. 1998; 160: 325-9.
- Tobias-Machado M, Pinto MA, Juliano RV, Borrelli M, Wroclawski ER: Extraperitoneal laparoscopic access: experience in 72 cases. Int Braz J Urol. 2001; 27 (suppl 2): 121-122 [in Portuguese].
- Wichkam JEA: The Surgical Treatment of Renal Lithiasis. In: Wickham JEA, (ed.), Urinary Calculous Disease. New York, Churchill Livingstone. 1979; pp. 145-198.
- Gaur DD: Laparoscopic operative retroperitoneoscopy: use of a new device. J Urol. 1992; 148: 1137-9.
- Gill IS, Schweizer D, Hobart MG, Sung GT, Klein EA, Novick AC: Retroperitoneal laparoscopic radical nephrectomy: the Cleveland Clinic experience. J Urol. 2000; 163: 1665-70.
- Gill IS, Rassweiler JJ: Retroperitoneoscopic renal surgery: our approach. Urology. 1999; 54: 734-8.
- Gill IS, Clayman RV, Albala DM, Aso Y, Chiu AW, Das S, et al.: Retroperitoneal and pelvic extraperitoneal laparoscopy: an international perspective. Urology. 1998; 52: 566-71.
- Tobias-Machado M, Pinto MA, Juliano RV, Cintra CC, Wroclawski ER: Retroperitoneoscopic renal biopsy. Int Braz J Urol. 2002; 28: 192-6.
- Suzuki K: Laparoscopic adrenalectomy: retroperitoneal approach. Urol Clin North Am. 2001; 28: 85-95.
- Hemal AK, Gupta NP, Wadhwa AG, Kumar R: Retroperitoneoscopic nephrectomy and nephroureterectomy for benign nonfunctioning kidneys: a single-center experience. Urology. 2001; 57: 644-9.
- Hemal AK, Wadhwa SN, Kumar M, Gupta NP: Transperitoneal and retroperitoneal laparoscopic nephrectomy for giant hydronephrosis. J Urol. 1999; 162: 35-9.
- Gill IS, Munch LC, Lucas BA: Initial experience with retroperitoneoscopic nephroureterctomy: use of a double-ballon technique. Urology. 1995; 46: 747-50.
- Tobias-Machado M, Pinto MA, Juliano RV, Mattos MHE, Wroclawski ER: Alternatives for distal ureter resection in laparoscopic nephroureterectomy. Int Braz J Urol. 2002; 28: 109-15.
- Gill IS, Grune MT, Munch LC: Access technique for retroperitoneoscopy. J Urol. 1996; 156: 1120-4.
- Tobias-Machado M, Pinto MA, Juliano RV, Borrelli M, Wroclawski ER: Preliminary results of ureteral intussuception in exclusive retroperitoneoscopic nephroureterectomy. Acta Esp Urol. 2002; 55: 582-6.
- Tobias-Machado M, Cartum J, Santos-Machado TM, Gaspar HA, Simões AS, Cruz R: Retroperitoneoscopic adrenalectomy in an infant with adrenocortical virilizing tumor. São Paulo Med J. 2002; 120: 87-9.
- Matin SF, Gill IS: Laparoscopic radical nephrectomy: retroperitoneal versus transperitoneal approach. Curr Urol Rep. 2002; 3: 164-71.
- Wolf JS Jr, Monk TG, McDougall EM, McClennan BL, Clayman RV: The extraperitoneal approach and subcutaneous emphysema are associated with greater absorption of carbon dioxide during laparoscopic renal surgery. J Urol. 1995; 154: 959-63.
- Janetsckek G, Peschel R, Franscher F: Laparoscopic pyeloplasty. Urol Clin North Am. 2000; 27: 695-704.
- Hobart MG, Schweizer D, Gill IS: Bilateral retroperitoneal laparoscopic nephrectomy for adult polycistic kidney disease. J Endourol. 1999; 13 (suppl 1): 90-1.
____________________
Received: April 14, 2003
Accepted after revision: August 26, 2003
_______________________
Correspondence address:
Dr. Marcos Tobias-Machado
Rua Oscar Freire, 1546 / 53
São Paulo, SP, 05409-010, Brazil
Fax: + 55 11 3887-3363
E-mail: telmamsm@icrhcnet.usp.br