FULL-THICKNESS
ABDOMINAL SKIN GRAFT FOR LONG-SEGMENT URETHRAL STRICTURE RECONSTRUCTION
(
Download pdf )
JOSHUA J. MEEKS, BRADLEY A. ERICKSON, CHRIS M. GONZALEZ
Department of Urology, Northwestern University, Feinberg School of Medicine, Chicago, Illinois, USA
ABSTRACT
Multiple tissue sources have been used for urethral reconstruction in adults. Patients with lichen sclerosis (LS), long segment strictures, or prior oral graft use have less available tissue for urethroplasty. We describe a technique for the use of a full-thickness skin graft of hairless abdominal skin for long segment urethroplasty.
Key
words: skin grafting, urethroplasty
Int Braz J Urol. 2008; 34: 602-8
INTRODUCTION
Reconstruction of long-segment adult urethral stricture disease as a result of lichen sclerosis (LS) or failed pediatric hypospadias repair remains a difficult urological problem mainly due to the deficiency of available extra-genital skin for grafting (1). Graft tissue has been utilized successfully for urethral reconstruction from various sites including buccal mucosa, genital skin and auricular tissue; however each tissue source has specific drawbacks (2). The ideal graft source would be extra-genital in origin, hairless, produce minimal postoperative morbidity at the harvest site, be inconspicuous postoperatively and abundant enough in length and width so as to avoid multiple urethral suture lines for men with long segment strictures. In an effort to develop an alternative to available graft sources for complex and long-segment strictures we describe harvest and application of a full-thickness abdominal skin graft for urethral reconstruction.
SURGICAL TECHNIQUE
The
extent of the urethral stricture was evaluated preoperatively with cystoscopy
and retrograde urethrogram. The area of abdominal wall to be harvested
was demarcated and discussed with the patient preoperatively. Deep venous
thrombosis precautions were taken, and all patients achieved a sterile
urine culture prior to surgery.
For one or two-staged long segment urethral
reconstructive procedures involving the mid or proximal bulbar urethra,
the patient was placed in the low lithotomy position. Otherwise, those
with stricture confined to the penile urethra and distal bulbar urethra
were placed in the supine position. A ventral longitudinal shaft incision
is made to expose the penile urethra to the level of the scrotum in men
undergoing single-staged repair with a perineal counter-incision to access
the bulbar urethra if needed. A bougie-à-boule sound is then used
to identify the anatomically distal most aspect of the stricture. The
urethra is incised along its anterolateral edge throughout the length
of the stricture with the edges of the urethrotomy calibrated to 24 F
in the penile urethra and 26F for the bulbar urethra. The full extent
of the urethrotomy is then measured in preparation for graft harvest.
Alternatively, in men undergoing the first of a two-staged procedure for
long segment stricture disease, a grooved director is placed within the
urethra and a scalpel is used to open the urethra through the full thickness
of the penile skin and urethra. The mucosa from the proximal urethrotomy
site is then sutured to the overlying penile, scrotal, or perineal skin,
depending on stricture length, with interrupted 5-0 vicryl sutures. All
nonviable corpus spongiosum and urethral mucosa or tissue that is suspicious
for lichen sclerosis is excised and sent for pathologic analysis in both
single and two staged procedures.
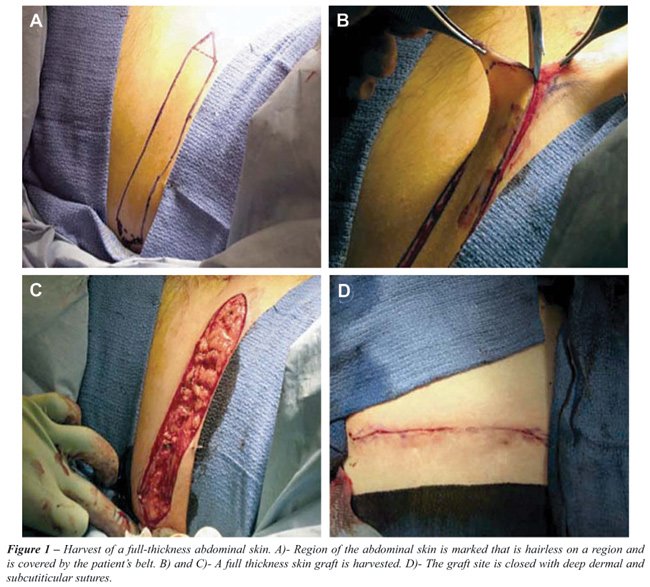
Graft harvest of the abdominal wall involves
excision of the skin of the right or left lower quadrant of the abdomen
at the level of the anterior superior iliac crest (Figure-1). An area
of hairless skin is identified and chosen in a location which is anatomically
positioned so that the patient’s belt line will eventually conceal
the wound (Figure-1A). A full thickness skin graft is harvested to the
level of the subcutaneous tissue (Figure-1B and Figure-1C). Once the graft
is sharply excised, the deep dermal tissue of the harvest site is closed
with interrupted 3-0 vicryl sutures followed by a 4-0 vicryl subcuticular
skin closure (Figure-1D). The graft is then prepared by sharp dissection
over its dermal edge until transparent (Figure-2A).

For single-stage procedures, the epithelial
side of the graft is sutured to the remaining mucosa of the urethral plate
with 5-0 vicryl suture. In the first of a two-staged procedure, graft
fixation to the dartos fascia is accomplished by suturing the graft to
the urethral plate medially and the penile skin laterally (Figure-2B).
Venting incisions or “pie crusting” is then completed through
the graft, and quilting sutures are placed per square centimeter in order
to fix the graft to the underlying dartos and corpora cavernosum to enhance
inosculation and prevent sub-graft fluid collections (Figure-2B).
A 16F catheter is left in place for strictures
limited to the penile urethra and an 18F catheter is placed for strictures
extending into the bulbar urethra. All men undergoing the first of a two-staged
procedure had a catheter placed for 5 days postoperatively in conjunction
with a moisturized bolster dressing. All other patients undergoing a single
procedure for repair had catheter drainage for three weeks postoperatively.
RESULTS
Abdominal
skin was used in ten patients with long-segment urethral stricture disease
(Table-1). Median patient age was 42 years (range 18-77 years). Mean stricture
length was 12 cm (range 10-24 cm). The etiology of urethral stricture
included failed hypospadias repair (2), LS (6) and unknown (2). Median
follow-up was 17 months (range 3-25 months). Average graft area was 42.25
cm2. Six of the ten patients underwent two-staged procedures
with successful graft uptake in all men after the first stage and successful
second stage closure in the two men completing both procedures (Figure-3A
and Figure-3B). In the other four men, strictures were closed in one stage
with a long segment graft. Mean estimated blood loss was 412 cc. Two patients
with LS developed recurrent stricture formation at a mean time of 9 months
from surgery. These were the first two patients in this series with prior
urethroplasty utilizing buccal and auricular tissue and involved stricture
lengths of 21 and 24 cm. Recurrent stricture length was 2 cm in each patient
and was managed endoscopically.

All abdominal skin harvest sites healed
well without complication. Two patients developed febrile urinary tract
infections requiring oral antibiotics. Two patients grew hair from segments
of the abdominal skin graft within six months of surgery, one after single
stage urethroplasty and the other after the first of a two-staged procedure.
These were the first two grafts harvested in this series when areas with
hair were taken and the follicles removed. This method proved to be unsuccessful
in its ability to prevent all future hair growth, and all subsequent grafts
were harvested from hairless abdominal regions with no further occurrences
of hair growth on the graft. All patients in this series were discharged
on postoperative day one and reported minimal pain at the abdominal harvest
site.
COMMENTS
Urethral
reconstruction in patients with long segment stricture disease remains
a complicated surgical problem especially in men with previous hypospadias
surgery and those with LS as an etiology. The success rates of reconstruction
in men with longer segment strictures of varied etiology has been reported
to be 75% at five years with a median stricture length of 7cm (3). Urethral
reconstruction for long segment stricture disease after previous hypospadias
repair has a similar 75% success rate at nearly three years (4). Men with
long-segment stricture disease secondary to LS appear to have a higher
recurrence rate secondary to the progressive nature of this inflammatory
disorder.
One of the critical events for urethral
reconstruction of long-segment strictures involves obtaining the appropriate
tissue for urethral defect substitution. Harvest of tissue from the surrounding
penile skin is ideal, but this tissue is often deficient, scarred, or
may be at risk for recurrence of LS. To repair long-segment defects, some
authors have used composite repairs including genital fasciocutaneous
flaps in conjunction with buccal or penile skin grafts. Berglund and Angermeir
described the use of a combined penile or scrotal skin flap with buccal
mucosa grafts in patients with strictures up to 24 cm in length with a
success rate of 83% approaching 6 years of follow-up (5). While these
authors were able to obtain good results from these techniques for long-segment
strictures some of the potential drawbacks include the need to harvest
graft tissue from multiple sites, the risk of suture line ischemia secondary
to incorporation of multiple grafts into the anastomosis, the risk of
hair growth on genital graft or flap tissue, and utilization of genital
skin which may predispose to an LS related stricture recurrence.
Buccal mucosa alone has been demonstrated
to be a good choice for extra-genital graft tissue with success rates
reaching 90% in some series. However, a significant limitation of buccal
mucosa for substitution in long segment stricture reconstruction involves
the availability of this tissue. The cumulative length of available oral
mucosa is approximately 17 cm which requires harvest from both cheeks
and potentially the lower lip. Complications reported with oral harvest
from just one site include neurosensory deficits, changes of salivary
flow, difficulty with mouth opening, and lip contracture (5,6). In one
report, as many as 26% of men indicated negative or mixed feelings about
the buccal mucosa graft harvest postoperatively with 16% reporting persistent
numbness and 32% reporting oral tightness (2). Comparatively, we experienced
no harvest site morbidity and limited patient complaints related to the
abdominal wall harvest for long-segment strictures with a mean length
of 12 cm.
The use of non-oral, extra-genital FTSG
has previously been described in several smaller series for urethral reconstruction
with reported success ranging from 25-50% (7). These outcomes may have
been related, in part, to the widespread use of tube-grafts for reconstruction
at this time, and the choice of single versus two-staged repair for complicated
strictures. The use of full-thickness abdominal wall skin for long-segment
stricture reconstruction has not been described previously. The advantages
of this tissue are that it provides extra-genital tissue origin, the ability
to harvest hairless segments up to 24 cm, and the limited graft site morbidity
observed in this series. Furthermore, the abundant length and width of
the abdominal skin graft allows for harvest of a single graft segment
as compared to buccal mucosa or penile skin grafts which require multiple
harvest sites and suture lines between grafts within an anastomosis for
long-segment stricture defects. While abdominal skin tissue should not
be the first choice for graft tissue until long-term outcomes are known,
the availability of this tissue offers the reconstructive surgeon an additional
option for substitution urethroplasty of long-segment strictures.
CONCLUSION
We describe a technique for full-thickness abdominal skin graft use in long-segment urethral stricture reconstruction. When harvested from hairless regions, these grafts have acceptable success rates with few complications at early follow-up. Selective use of abdominal skin grafts may be well suited for patients with long-segment urethral strictures in one or two stages when other graft sources are not available or feasible.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Xu YM, Qiao Y, Sa YL, Wu DL, Zhang XR, Zhang J, et al.: Substitution urethroplasty of complex and long-segment urethral strictures: a rationale for procedure selection. Eur Urol. 2007; 51: 1093-8; discussion 1098-9.
- Dublin N, Stewart LH: Oral complications after buccal mucosal graft harvest for urethroplasty. BJU Int. 2004; 94: 867-9.
- Moradi MR, Moradi A: Urethroplasty for Long Anterior Urethral Strictures: Report of Long-term Results. Urol J. 2006; 3: 160-4.
- Barbagli G, De Angelis M, Palminteri E, Lazzeri M: Failed hypospadias repair presenting in adults. Eur Urol. 2006; 49: 887-94; discussion 895.
- Berglund RK, Angermeier KW: Combined buccal mucosa graft and genital skin flap for reconstruction of extensive anterior urethral strictures. Urology. 2006; 68: 707-10; discussion 710.
- Jang TL, Erickson B, Medendorp A, Gonzalez CM: Comparison of donor site intraoral morbidity after mucosal graft harvesting for urethral reconstruction. Urology. 2005; 66: 716-20.
- Webster GD, Brown MW, Koefoot RB Jr, Sihelnick S: Suboptimal results in full thickness skin graft urethroplasty using an extrapenile skin donor site. J Urol. 1984; 131: 1082-3.
____________________
Accepted after revision:
June 4, 2008
_______________________
Correspondence address:
Dr. Chris M. Gonzalez
Northwestern University
Feinberg School of Medicine
675 North St. Clair Street, Galter 20-150
Chicago, IL, 60611, USA
E-mail:j-meeks@md.northwestern.edu
EDITORIAL COMMENT
The
authors reported on the use of full-thickness abdominal skin graft for
urethral strictures as an “inlay” after extensive urethrotomy
for long strictures. The paper was submitted as an operative technique
description focusing mainly in the procedure itself with a limited number
of patients treated (10) and only 6 completing the second-stage. Follow-up
is also very short (17 months).
The paper has some merit but adds little
to the present knowledge in urethroplasty. Since the popularization of
mucosal grafts in urethral structure and hypospadias repair, there is
a consensus that mucosal grafts are more appropriate and recently tunica
vaginalis is also being studied as a valid option. Skin grafts have been
extensively studied in the past with success and reported in the literature
also with long term follow-up. Bracka has shown long-term clinical data
in over 1000 patients with skin grafts and later buccal mucosa grafts
including the second-stage urethroplasty. The argument of the authors
that the suggested donor area is attractive should be based on clinical
results in a larger series and not only on surgical technique descriptions.
In summary, I would like to encourage the
authors to resubmit their experience later with more patients and a longer
follow-up.
Dr.
Antonio Macedo Jr.
Federal University of Sao Paulo
Sao Paulo, SP, Brazil
E-mail: amcdjr@uol.com.br
REPLY BY THE AUTHORS
In this surgical technique manuscript, we describe the procedure to harvest, prepare and place a full-thickness skin graft for men with long segment urethral strictures. While long segment urethral reconstruction is relatively rare, the most difficult part of urethroplasty is finding an ideal tissue source for urethral reconstruction. Many have described the use of genital skin, non-genital skin and buccal mucosa as graft sources; these standard tissues sources are often deficient in men with prior urethroplasty or pediatric hypospadias repair, as several men in our study were. In our study, the mean stricture length was 12 cm with a range of 10 to 24 cm. In this population, the potential graft sources include composite grafts of multiple buccal grafts with the possible addition of skin grafts. Yet, almost 25% of men describe a complication after buccal harvest. The technique we describe is not meant to replace standard techniques of buccal or genital skin grafts, but is a supplemental technique to consider when approaching a complicated patient with few ideal graft sources. As the editor mentions, more data will be forthcoming.
The Authors