THE
ROLE OF EXTENDED PROSTATE BIOPSY ON PROSTATE CANCER DETECTION RATE: A
STUDY PERFORMED ON THE BENCH
(
Download pdf )
LUCIANO NESRALLAH, ADRIANO NESRALLAH, ALBERTO A. ANTUNES, KATIA R. LEITE, MIGUEL SROUGI
Division of Urology, University of Sao Paulo Medical School, USP, Sao Paulo, SP, Brazil
ABSTRACT
Introduction:
The aim of this prospective study was to compare the advantage of performing
prostate biopsy with a greater number of cores using the classic sextant
procedure, with the aim of reducing false negative results.
Materials and Methods: 100 prostates were
acquired from consecutive radical prostatectomies performed by the same
surgeon. Fourteen cores were obtained on the bench following surgery using
an automatic pistol with an 18-gauge needle. Six of these cores were obtained
according to the sextant technique, as described by Hodge et al.; with
the addition of a further three lateral cores from each lobe and one from
the bilateral transition zone. The whole gland and the fragments were
assessed by the same pathologist. An analysis of the frequency of the
cancers identified in the cores of the sextant and the extended biopsies
was undertaken and the results evaluated comparatively. The chi-square
test was used for the comparative analysis of the cancer detection rate,
according to the technique used.
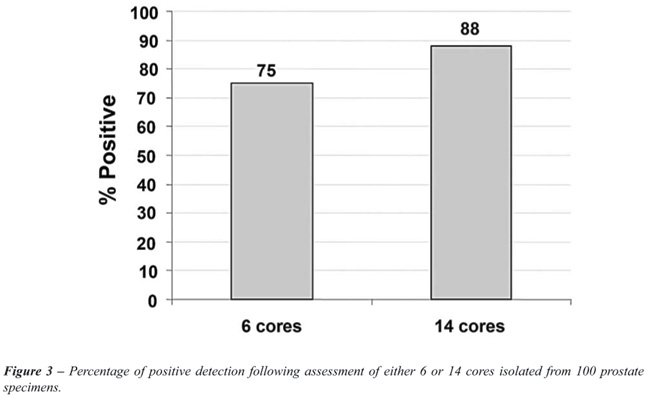
Results: When 6 cores were removed, the
positive cancer rate was 75%, which was increased to 88% when 14 cores
were (p < 0.001). The withdrawal of 14 cores resulted in a significant
13% (95% CI [5%-21%]) increase in the positive rate of cancer detection.
Conclusion: Extended biopsy, with the removal
of 14 cores, is more efficient than the sextant procedure in improving
the rate of prostate cancer detection.
Key
words: prostatic neoplasm; biopsy needle; pathology; diagnosis
Int Braz J Urol. 2008; 34: 563-71
INTRODUCTION
Prostate
cancer is the most common non-cutaneous malignant tumor in men. In the
United States, it accounts for 33% of all new cancer cases and it is estimated
that 218,890 men will be diagnosed in 2006, 91% of which will be discovered
at a localized or regional stage. Moreover, it is estimated that 27,050
men will die of the disease (1).
A great challenge for the early diagnosis
of prostate cancer is that in its initial phase, the tumor is asymptomatic
and only detected by the alterations in the digital rectal examination,
abnormal increase in the plasma level of the prostate specific antigen
(PSA) or by means of transrectal ultrasound revealing hyperechoic and
hypervascularized areas. When any of these alterations is found, it becomes
necessary to perform a transrectal ultrasound-guided prostate biopsy.
In 1989, Hodge and colleagues proposed the
undertaking of routine sextant biopsy and demonstrated the superiority
of the method compared to the digitally guided biopsy directed to nodules
or suspected areas. This method has become the gold standard for the diagnosis
of prostate cancer (2).
A study with a mathematical laboratory model
showed that sextant biopsy could detect the tumor in 36%, 44% and 100%
of the cases in which the lesion occupied 2.5%, 5% and 20%, respectively,
of the gland volume (3). However, the sextant biopsy has led to false
negative results in 15% to 34% of men (4-7). Furthermore, the general
sensitivity of the sextant biopsy was only 60% in patients with normal
prostatic DRE (8).
For these reasons, various modifications
of the technique have been proposed, some of which suggested the acquisition
of cores in a more lateral region (9) or an increase in the number of
cores obtained (10-13). There seems to be a consensus in the literature
as to the superiority of the techniques that involve the withdrawal of
a larger number of cores for the diagnosis of adenocarcinoma of the prostate
(10,12,14). However, the number of cores to be obtained varies significantly
among the various studies published, with no overall consensus. In reviewing
the subject, we found only one prospective and randomized study that compared
6 and 12-core biopsies obtained in a significant number of patients (14).
This study did not demonstrate any significant difference between the
two procedures in the detection of prostate cancer.
Curiously, recent analyses have shown that
in the United States and the United Kingdom, traditional sextant biopsy
continues to be used in 20% to 70% of the diagnostic centers, demonstrating
a general uncertainty as to the ideal number of cores to be obtained in
prostate biopsy (15-17). In the studies that show advantages from the
removal of more than 6 cores, the comparison of sextant with extended
biopsy was performed in groups of patients suspected of having of prostate
cancer. To examine the true incidence of false negative results, it would
be necessary to obtain the biopsy on patients known to be bearers of the
disease (i.e., those with a previous positive biopsy). Further, the withdrawal
of a large number of cores could lead to an increase in the diagnosis
of tumors of no clinical importance and requiring no treatment. This question
could only be answered if the entire prostate were examined histologically
and completely, thus permitting the definition of the pathological characteristics
of the tumor.
This study compares the rates of prostate
cancer detection by means of the withdrawal of 6 or 14 cores in order
to determine the cancer detection rates of the two techniques.
MATERIALS AND METHODS
The
study comprised of a prospective and controlled analysis of prostate glands
obtained by radical prostatectomy of one hundred consecutive patients
with clinically localized prostate cancer during the period of August
2000 to March 2001. The project was approved by the Ethics in Research
Committee of the hospital.
All the operations were performed by the
same surgeon (MS), in accordance with the surgical technique previously
described.
The inclusion criteria were the presence
of adenocarcinoma of the prostate in clinical stages T1-T2 and recommendation
of radical prostatectomy. Patients with a previous history of radiotherapy,
hormone therapy or transurethral removal of the prostate were excluded.
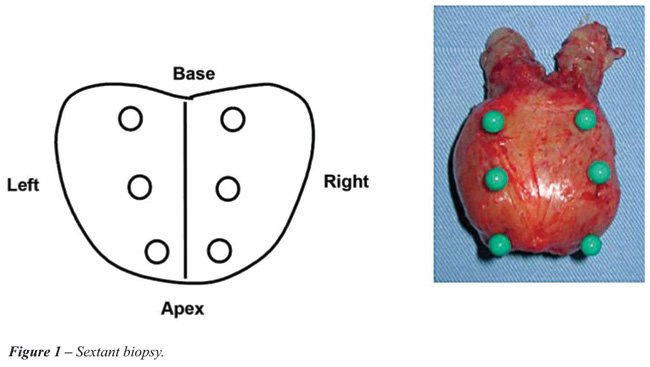
All the surgical specimens were subjected
to biopsy on the bench, immediately after their removal with an 18-gauge
needle and an automatic pistol. Six cores were obtained from the peripheral
zone, one from each sextant, according to Hodge et al. and were identified
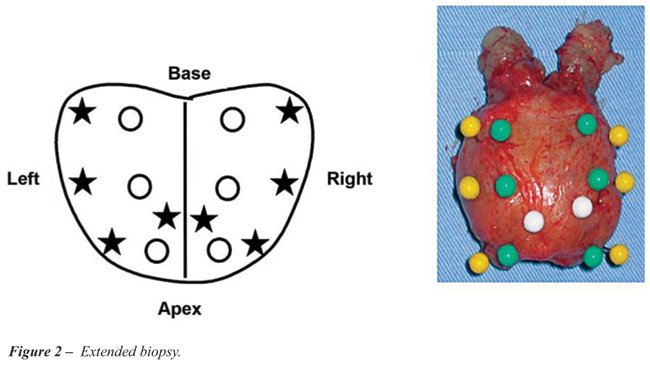
and analyzed under the label sextant biopsy (2). An additional 8 cores
were then removed, three from the peripheral zone of the most lateral
edge of the prostate and one core from the transitional zone of each lobe
(Figures-1 and 2). These cores were analyzed together with the first 6
(a total of 14 cores) and were labeled as extended biopsy. All the cores
were stored in separate flasks and sent, together with the surgical specimens,
for pathological analysis. The histological reading of all the slides
was carried out by the same pathologist (KRL).
The biopsy cores and the surgical specimens
were fixed in 10% formalin for a period of 4 to 16 hours. All the glands
were submitted to histological study in accordance with the recommendations
previously described (18).
Both the biopsy cores and the surgical specimens
were investigated for the presence of adenocarcinoma, as classified in
accordance with Gleason’s criteria (19).
The chi-square test was used for the comparison
of the frequency of the positive results in both the sextant and the extended
biopsies, employing a 95% confidence interval (95% CI) for each value.
A 5% significance level (p < 0.05) was adopted for the rejection of
the null hypothesis.
RESULTS
The
determined positive cancer rate was compared between the groups of the
sextant and extended biopsies. Each of the specimens assessed was considered
to be positive when at least one positive core was found in the sample.
Table-1 shows the joint distribution of the 100 assessed specimens when
six and 14 cores were analyzed.
It may be observed from Table-1 that when
6 cores were removed the positive cancer rate was of 75%, compared to
a rate of 88% when 14 cores were removed. Results of McNemar`s chi-squared
test showed that there was a difference in the positive detection rate
between these two techniques (p < 0.001). Thus, when 14 cores were
removed there was a significant increase in the positive cancer detection
rate (Figure-3), estimated at 13% (95% CI [5% - 21%]).
Cancer detection in each group increased
as PSA increased but there was no significant difference between the groups
(Table-2).
COMMENTS
Transrectal
ultrasound-guided biopsy is the procedure of choice for the diagnosis
of prostate cancer when the disease is suspected due to alterations in
the PSA levels and/or alterations perceived by the DRE. This method has
been modified, as there has recently been a tendency to obtain more than
8 cores, despite a lack of standardized literature on the subject. Regardless
of recent studies demonstrating that extended biopsy fails less often
in the diagnosis of prostate adenocarcinoma compared to the classic sextant
biopsy proposed by Hodge et al., a large number of clinics still prefer
the sextant technique. Although no data on this subject has been reported,
we observed that the majority of clinics continue to follow the sextant
method and biopsy only 6 cores. In our study, we were able to demonstrate
that 6 cores biopsy fails in 25% of the cases, while taking 14 cores decreases
the failure rate to 12%, i.e. it detects 50% more.
When the 25 prostates, where the sextant
biopsy was negative, were further analyzed, it was observed that the tumor
was confined in 72% of them. Although no tumors were found in any of the
cores, the disease was already extraprostatic in 28% of the cases. Conversely,
in those cases where no tumor was found in the 14-core biopsy, only 8.3%
of the specimens showed non-localized disease.
The fact that the present study was undertaken
on 100 prostates acquired from consecutive radical prostatectomies not
only eliminates any possible bias in the selection of cases, but also
allowed us to compare the results of the two different methods applied
to the same specimens. This differentiates this study from previous reports,
all of which compared the findings of sextant biopsy with those of extended
biopsy, undertaken “in vivo”, and therefore, on different
patients. Another advantage in using surgical specimens on the bench is
that the procedure permits the acquisition of cores of better quality
from more precise locations, as well as being undertaken by the same investigator,
which is in contrast to the published studies in which the biopsy may
be taken by different doctors, introducing a possible bias. Another strength
of this study is that all the operations were carried out by the same
surgeon, as well as all the pathological evaluation was performed by the
same uropathologist, thus avoiding the inter-observer differences that
are well-known in the literature.
Because it is intuitive, it is easy to accept
that an increase in the number of cores obtained in a prostate biopsy
will result in an improvement in the detection rate for prostate cancer.
However, there is only indirect evidence and that expectation has not
yet been completely proven by scientific studies. For example, the same
author suggests opposite results. Naughton and colleagues first showed
that 44% of cancer diagnoses require a biopsy from 7 to 13 cores, in a
retrospective analysis (20). Later in a prospective study these authors
showed that there was no statistically significant difference in the diagnosis
of prostate adenocarcinoma when 6 and 12-core biopsies were compared (14).
Studies undertaken on Japanese men showed a much smaller improvement of
7.7% to 13.8% when 12 cores were obtained, as compared to those demonstrated
by western studies (21,22). In a prospective study, in which 6 and 12-core
biopsies by transperineal approach were compared, no significant difference
was found when a palpable nodule or lesion suspected by transrectal ultrasound
existed, except in situations in which there was an increase in the level
of PSA with no alteration in the DRE or ultrasound, when the 12-core biopsy
demonstrated an advantage (23). One variable that may affect the results
of the biopsy is the volume of the prostate. Cancer detection in prostates
less than 50 cc was 38%, whereas prostates more than 50 cc have a lower
detection rate (23%) (24). One randomized prospective study investigated
the influence of the increase in the number of cores as a function of
prostate volume. In patients with no palpable nodule but increased PSA
levels, the cancer detection rate doubled when using biopsies of 10 to
14 cores compared to the sextant technique (25). This correlation involving
the need to increase the number of biopsy cores in accordance with the
volume of the prostate has also been found in a Turkish study, in which
the authors suggest that the sextant biopsy was not reliable even in small
prostates. The study further recommended that prostates of more than 35
cc should have 10 cores removed, and that in smaller glands only 8 cores
need to be obtained (26). The same author had previously demonstrated,
though without relating the number of cores to prostate volume, that when
10 cores were obtained the cancer detection rate increased by 25.5% as
compared with the classic 6-core biopsy (27). In the present study the
average weight of the prostates was of 42.4 cc, the standard deviation
was 23.9 cc, and the increase in tumor detection was of 13% when 14 cores
were used compared with a 6-core biopsy.
In another study of 179 consecutive patients
who underwent radical prostatectomy, it was observed that a 12-core biopsy
detected 31.3% more cancer than the sextant technique (28). A group from
the University of Vienna working with Athenian urologists in the attempt
to validate a nomogram to define the ideal number of biopsy cores based
on the age and prostate volume of the patient, submitted 502 men to biopsy
on the basis of the criteria of the nomogram. The results were then compared
with those of a control group of 1,051 patients who had previously had
octant biopsy and re-biopsy when the former was negative. The disease
was found in 36.7% of the patients when the Vienna nomogram was used,
compared with 22% at the first octant biopsy and 10% on re-biopsy (29).
This group confirmed that the sextant biopsy should only be used on patients
of more than 70 years of age, who have a prostate volume of less than
40 mL. After excluding that group of patients, the techniques that used
at least 8 core samples was preferred, with the number of samples increasing
in accordance with the increased weight of the gland and as the age of
the patient diminished.
More recently, the possibility of using
the so-called saturation biopsies, which involve the withdrawal of more
than 18 cores, has been analyzed. In one study, 24 cores were each acquired
from 139 selected men and the procedure was performed by two surgeons.
The results were compared with a group of 87 patients who had previously
undergone the 10-core technique. No significant difference was found in
the detection of the disease between these two groups. The authors concluded
that a 10- or 12-core biopsy should be the method of choice for the first
investigation in the early detection of prostate cancer (30). This type
of strategy was also confirmed more recently in a systematic review of
the literature, by which the present authors arrived at the conclusion
that an investigation into prostate cancer using the 12-core biopsy should
be considered (31).
On the basis of our findings and also on
those reported in the literature, the authors suggest that there is no
longer any justification, in practice, for the continued use of the sextant
biopsy. Even with the extended technique, we still find an unacceptable
number of biopsies with false negative results (12%, according to our
data). In a future study we intend in to compare the extended with the
saturation biopsy on the bench, which involves the acquisition of more
than 18 cores, in an attempt to discover whether there is any advantage
in this latter method in the detection of adenocarcinoma of the prostate.
CONCLUSION
Extended biopsy, with the removal of 14 cores, could be considered more effective than the sextant procedure in improving the prostate cancer detection rate.
CONFLICT OF INTEREST
None declared.
REFERENCES
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ: Cancer statistics, 2007. CA Cancer J Clin. 2007; 57: 43-66.
- Hodge KK, McNeal JE, Terris MK, Stamey TA: Random systematic versus directed ultrasound guided transrectal core biopsies of the prostate. J Urol. 1989; 142: 71-4; discussion 74-5.
- Feneley MR, Parkinson MC: Biopsy diagnosis of prostatic cancer--current areas of concern. J Clin Pathol. 1997; 50: 265-6.
- Chen ME, Troncoso P, Johnston DA, Tang K, Babaian RJ: Optimization of prostate biopsy strategy using computer based analysis. J Urol. 1997; 158: 2168-75.
- Ellis WJ, Brawer MK: Repeat prostate needle biopsy: who needs it? J Urol. 1995; 153: 1496-8.
- Keetch DW, Catalona WJ, Smith DS: Serial prostatic biopsies in men with persistently elevated serum prostate specific antigen values. J Urol. 1994; 151: 1571-4.
- Norberg M, Egevad L, Holmberg L, Sparén P, Norlén BJ, Busch C: The sextant protocol for ultrasound-guided core biopsies of the prostate underestimates the presence of cancer. Urology. 1997; 50: 562-6.
- Terris MK: Sensitivity and specificity of sextant biopsies in the detection of prostate cancer: preliminary report. Urology. 1999; 54: 486-9.
- Stamey TA: Making the most out of six systematic sextant biopsies. Urology. 1995; 45: 2-12.
- Eskew LA, Bare RL, McCullough DL: Systematic 5 region prostate biopsy is superior to sextant method for diagnosing carcinoma of the prostate. J Urol. 1997; 157: 199-202; discussion 202-3.
- Levine MA, Ittman M, Melamed J, Lepor H: Two consecutive sets of transrectal ultrasound guided sextant biopsies of the prostate for the detection of prostate cancer. J Urol. 1998; 159: 471-5; discussion 475-6.
- Presti JC Jr, Chang JJ, Bhargava V, Shinohara K: The optimal systematic prostate biopsy scheme should include 8 rather than 6 biopsies: results of a prospective clinical trial. J Urol. 2000; 163: 163-6; discussion 166-7.
- Babaian RJ, Toi A, Kamoi K, Troncoso P, Sweet J, Evans R, et al.: A comparative analysis of sextant and an extended 11-core multisite directed biopsy strategy. J Urol. 2000; 163: 152-7.
- Naughton CK, Miller DC, Mager DE, Ornstein DK, Catalona WJ: A prospective randomized trial comparing 6 versus 12 prostate biopsy cores: impact on cancer detection. J Urol. 2000; 164: 388-92.
- Davis M, Sofer M, Kim SS, Soloway MS: The procedure of transrectal ultrasound guided biopsy of the prostate: a survey of patient preparation and biopsy technique. J Urol. 2002; 167: 566-70.
- Patel HR, Lee F, Arya M, Masood S, Palmer JH, Sheriff MK: A national survey of transrectal ultrasound-guided prostatic biopsies: time for a national guideline. Int J Clin Pract. 2003; 57: 773-4.
- Eichler K, Hempel S, Wilby J, Myers L, Bachmann LM, Kleijnen J: Diagnostic value of systematic biopsy methods in the investigation of prostate cancer: a systematic review. J Urol. 2006; 175: 1605-12.
- Bostwick DG, Foster CS: Examination of Radical Prostatectomy Specimens: Therapeutic and Prognostic Significance. In: Foster CS, Bostwick DG (eds.) Pathology of Prostate. Philadelphia, WB Saunders. 1998; pp. 172.
- Gleason DF: Histologic grading of prostate cancer: a perspective. Hum Pathol. 1992; 23: 273-9.
- Naughton CK, Smith DS, Humphrey PA, Catalona WJ, Keetch DW: Clinical and pathologic tumor characteristics of prostate cancer as a function of the number of biopsy cores: a retrospective study. Urology. 1998; 52: 808-13.
- Matsumoto K, Satoh T, Egawa S, Shimura S, Kuwao S, Baba S: Efficacy and morbidity of transrectal ultrasound-guided 12-core biopsy for detection of prostate cancer in Japanese men. Int J Urol. 2005; 12: 353-60.
- Kojima M, Hayakawa T, Saito T, Mitsuya H, Hayase Y: Transperineal 12-core systematic biopsy in the detection of prostate cancer. Int J Urol. 2001; 8: 301-7.
- Emiliozzi P, Scarpone P, DePaula F, Pizzo M, Federico G, Pansadoro A, et al.: The incidence of prostate cancer in men with prostate specific antigen greater than 4.0 ng/ml: a randomized study of 6 versus 12 core transperineal prostate biopsy. J Urol. 2004; 171: 197-9.
- Uzzo RG, Wei JT, Waldbaum RS, Perlmutter AP, Byrne JC, Vaughan ED Jr: The influence of prostate size on cancer detection. Urology. 1995; 46: 831-6.
- Mariappan P, Chong WL, Sundram M, Mohamed SR: Increasing prostate biopsy cores based on volume vs the sextant biopsy: a prospective randomized controlled clinical study on cancer detection rates and morbidity. BJU Int. 2004; 94: 307-10.
- Eskicorapci SY, Guliyev F, Akdogan B, Dogan HS, Ergen A, Ozen H: Individualization of the biopsy protocol according to the prostate gland volume for prostate cancer detection. J Urol. 2005; 173: 1536-40.
- Eskicorapci SY, Baydar DE, Akbal C, Sofikerim M, Günay M, Ekici S, et al.: An extended 10-core transrectal ultrasonography guided prostate biopsy protocol improves the detection of prostate cancer. Eur Urol. 2004; 45: 444-8; discussion 448-9.
- Singh H, Canto EI, Shariat SF, Kadmon D, Miles BJ, Wheeler TM, et al.: Improved detection of clinically significant, curable prostate cancer with systematic 12-core biopsy. J Urol. 2004; 171: 1089-92.
- Remzi M, Fong YK, Dobrovits M, Anagnostou T, Seitz C, Waldert M, et al.: The Vienna nomogram: validation of a novel biopsy strategy defining the optimal number of cores based on patient age and total prostate volume. J Urol. 2005; 174: 1256-60; discussion 1260-1; author reply 1261.
- Jones JS, Patel A, Schoenfield L, Rabets JC, Zippe CD, Magi-Galluzzi C: Saturation technique does not improve cancer detection as an initial prostate biopsy strategy. J Urol. 2006; 175: 485-8.
- Eichler K, Hempel S, Wilby J, Myers L, Bachmann LM, Kleijnen J: Diagnostic value of systematic biopsy methods in the investigation of prostate cancer: a systematic review. J Urol. 2006; 175: 1605-12.
____________________
Accepted after revision:
March 3, 2008
_______________________
Correspondence address:
Dr. Miguel Srougi
Rua Peixoto Gomide, 2055/81
São Paulo, SP, 01409-003, Brazil
Fax: + 55 11 3257-9006
E-mail: srougi@terra.com.br
EDITORIAL COMMENT
It
is commonly accepted that traditional sextant transrectal biopsy may underestimate
the true tumor burden within the prostate after a whole mount specimen
is available. Today as technology continues to evolve, it is imperative
that clinicians have the most accurate and comprehensive information available
upon which to base their recommendations. We know from large retrospective
series of radical prostatectomies that traditional sextant biopsy may
underestimate the true tumor extent by as much as 46.6% when the whole
mount specimen is examined (1). The authors are to be commended on this
prospective analysis of 100 consecutive radical prostatectomy specimens
performed by the same surgeon and pathology reviewed by the same pathologist.
Previous investigators have demonstrated an increased yield of malignant
diagnoses in vivo using extended systematic sextant biopsy of twelve cores
versus traditional sextant biopsy (2). To my knowledge this study is unique,
based on the fact that the needle core biopsies were obtained from the
RP specimen on the bench.
Clearly, the author’s data demonstrate
a statistically significant increased yield of malignant diagnoses of
13% when additional lateral cores were obtained from each lobe and bilateral
transition zone. These results further support the current trend of extended
systematic sextant biopsy of 12-14 cores.
There is a subset of patients that will
have negative biopsies even with the additional lateral and transitional
cores, yet the PSA level may continue to rise. This particular scenario
presents a diagnostic dilemma to the clinician and anxiety for the patient.
In this setting, our approach is to perform stereotactic transperineal
prostate biopsy (STPB). Similar to a prostate brachytherapy procedure,
the prostate is positioned on the implant grid. Specimens are obtained
according to x, y, and z coordinates from eight equal octants with pathology
reported accordingly. Using this technique, we have consistently achieved
a 39% positive biopsy rate. There was a significant difference in detection
rates with the apex having a higher incidence of malignancy than the base
of the prostate gland (p = 0.000). Furthermore, the anterior apex harbored
significantly more adenocarcinoma when compared to the posterior apex
(p = 0.026) (3).
As our knowledge of biopsy techniques become
more sophisticated, it will be possible to map malignant versus benign
regions of the prostate; whether or not targeted focal therapy results
from this remains to be determined.
REFERENCES
- Fukagai T, Namiki T, Namiki H, Carlile RG, Shimada M, Yoshida H: Discrepancies between Gleason scores of needle biopsy and radical prostatectomy specimens. Pathol Int. 2001; 51: 364-70.
- Presti JC Jr, O’Dowd GJ, Miller MC, Mattu R, Veltri RW: Extended peripheral zone biopsy schemes increase cancer detection rates and minimize variance in prostate specific antigen and age related cancer rates: results of a community multi-practice study. J Urol. 2003; 169: 125-9.
- Moran BJ, Braccioforte MH, Conterato DJ: Re-biopsy of the prostate using a stereotactic transperineal technique. J Urol. 2006; 176: 1376-81; discussion 1381.
Dr.
Brian J. Moran
Medical Director, Radiation Oncology
Chicago Prostate Center
Westmont, Illinois, USA
E-mail: seeds@prostateimplant.com